Mechanisms of Hallucinations
By Heinrich Klover, 1912
The Castalia Foundation republishes the following article first published in 1912 (re-published in our magazine in 1966) purely to preserve the history of the magazine, and to satisfy the interest of the modern reader. The Psychedelic Review advises the modern reader that we are not enamored with the contents of this piece. We feel it is painfully dull, and myopically 'scientific'. We could say more, but we'll let the article speak for itself.
At the very least, we should warn you that the author seems to think that mescaline is 'poison'. In the author's defense, perhaps this was the inevitable position of most Western 'scientists', back in 1912. When encountering the thunderous magic of psychedelics, it is easier to cry 'poison' than to confront the strange and terrifying labyrinths of the soul.
The theories that have been evolved for an understanding of hallucinatory phenomena have frequently stressed one set of faction to the exclusion of others. They have stressed either psychological or physiological factors, 'peripheral' or 'central' factors, Sensory or motor factors, cortical or subcortical mechanisms.
In recent years, however, it has been generally recognized that all these factors are of importance. Since all of them are involved in any complex behavioral reaction, it is to be expected that they are involved in hallucinations. An investigator may insist, for instance, diat pathological changes in the lens of the eye in conjunction with certain psychological factors are primarily responsible for the appearance of a given hallucinatory phenomenon or that the combined orietts of vestibular dysfunction and a lesion of the occipital cortex determine another hallucinatory picture.
The fact that certain agent can be found which banish or provoke hallucinations does slot mean that the mechanisms involved in bringing about such a malt ale known. We know at present that hallucinations are influenced by a large number of widely different factors and that they wthibit a wide diversity of phenomenal characteristics.
Confronted with these etiological and phenomenal differences, we may ask. Whether it is possible at all to identify something like a general-structure in hallucinations or whether such a structure is disssolved by the operation of heterogeneous factors. In other words, there any hallucinatory constants? This question will be briefly discussed by utilizing certain findings in the literature as well as author's own studies in the field of eidetic phenomena and his ics of the effects produced by mescaline.
HALLUCINATORY CONSTANTS
Mescaline (3, 4, 5-trimethoxyphenethylamine) has been of unusual interest because of its remarkable psychological and physiological effects
[4, 7, 22. 32, 33, 41, 42, 52, 56, 75. 85]. Particularly the visual effects have been the subject of many studies, Veit and Vogt al,
[82] injected various alkaloids, including mescaline, into animals, which were then killed to determine the concentration of the poison in different parts of the central nervous system and in other tissues.
The amount of mescaline recovered from the occipital cortex of monkeys and clogs did not differ significantly from that found in the frontal cortex. As regards the effects on the optical sensorium, Maloney
[46] claimed that injections of mescaline sulfate led to an enormous enlargement of visual fields in "blind or nearly blind" tabetics and to an improvement in visual acuity, as measured by Snellen's test types.
Some of the patients were enabled to read who, previous to the injection, could not; one of them went to a motion-picture show. Recently Lidor
[88] reported that mescaline resored perception of movement in the hemianopic field of one of his patients (case 6). In this connection, the appearance of the "reddish-blue arcs" of the retina in the mescalinized state is of interest. It is generally agreed that these elliptical reddish-blue arcs, discovered by Purkinje
[64], correspond to fibers of the optic nerve, which become entoptically visible
[10, 40]. Normally, these area are very distinct for only a moment, but after an injection of mescaline sulfate the author noticed that they could be seen for a long time.
It is characteristic of the action of many drugs that visual effects predominate. Dominance of visual phenomena, a
traduzione visiva (
Sante de Sanctis), seems to be also typical of deliriums, dreams, and eidetic imagery. As regards the hallucinatory phenomena produced by mescaline, their chief character, according to Havelock Ellis, is their "indescribableness."
More than a decade ago, the author raised the question whether it was possible to find any constants in the flow of these "indescribable" experiences and analyzed the available data with reference to the jorm of the hallucinatory material.
[33] Investigators, such as Berze
[5], emphasizing the importance of motor, kinesthetic, or 'myopsychic' components in hallucinations, have called attention to the fact that most visual hallucinations are formed. There is no doubt that most reports on hallucinations refer to forms of some kind and not to the appearance of visual "dust" or similar material.
The author's amalysis of the hallucinatory phenomena appearing chiefly), during the first stages of mescaline intoxication yielded the following form constants:
- Grating; lattice; fretwork; filigree; honeycomb; chessboard.
- Cobweb.
- Tunnel, funnel, alley, cone, or vessel.
- Spiral.
Many phenomena are, on close examination, nothing but modifications and transformations of these basic forms, The tendency towards "geometrization," as expressed in these form constants, is also apparent in the following two ways:
- The forms are frequently repeated, combined, or elaborated into ornamental designs and mosaics of various kinds.
- The elements constituting these forms, such as the squares in a chessboard design, often have boundaries consisting of geometric forms.
At times, the boundaries are represented by lines so thin that it may be impossible to say whether they are black or white. Many observers have stressed the fineness of these lines, especially Ceroni
[6] and Moller
[54]. As Moller has pointed out, the "absolute one-dimensional" appears to have become a reality.
For the sake of analysis in terms of 'form', we have ignored aspects of color, brightness, and movement, but it is just these aspects which often deeply impress the subject and which he cannot adequately characterize when describing the kaleidoscopic play of forms and patterns. He may. for instance, claim that colors unknown in his previous experience appear; he may even be more impressed by the textures of colours — 'fibrous, woven, polished, glowing, dull, veined, semi-transparent'
[11], he may insist that the hallucinatory objects consist of materials that are never seen in nature and yet may strangely resemble certain kinds of wood, straw, hair, jewels, wool, silk, or marble.
If we ignore the colors and movements as well as the 'meaning' with which the phenomena are invested by the subject, the geometric-ornamental structure of the hallucinations becomes apparent, This appears even in the drawings made by artists during or after mescaline intoxication, Such drawings have been published by Szuman
[77], Marinesco
[48], and Maclay and Guttmann
[44].
The fact that certain geometric forms and designs constantly recur has led us to assume certain hallucinatory form constants. Although further analysis may reveal additional form constants, it seems certain that the number of basic forms is limited. At certain stages of the poisoning, the geometric forms and designs may be seen with open, as well as with closed, eyes, e.g. on the face of a person or on the soup the subject is about to eat.
It is significant that the tendency toward these forms may be so strong as to dominate the perception of external objects. One of Beringer's subjects looked at the small branch of a tree and reported:
"The leaves suddenly appeared in an ornamental pattern as if joined in a circular design, having the form of approximately a cobweb. I looked at other branches, and, looking at them, all leaves assumed the same lattice-like arrangement."[4]
Some or all of the form constants found in mescaline hallucinations are also found in certain hypnogogic hallucinations; in entoptic phenomena; in the visual phenomena of insulin hypoglycemia; and in phenomena induced by simply looking at disks with black, white, or colored sectors rotating at certain speeds
[9, 23, 49, 64, 84]. Occasionally they seem even to occur in fever deliriums.
One of the patients of Wolff and Curran
[86], who happened to be a trained observer and physician, reported that he observed the same hallucinatory phenomenon during four illnesses precipitated by four different agents (measles; malaria; tonsillitis; influenza) at the ages of 8, 12, 30, and 41, he saw a cloud "with a spiral motion shape itself into a brilliant whorl"
In two of these illnesses he saw that:
"brilliantly illuminated green, yellow and red angular crystalline masses shaped themselves into ever-changing patterns like those formed by bits of glass in a revolving kaleidoscope."
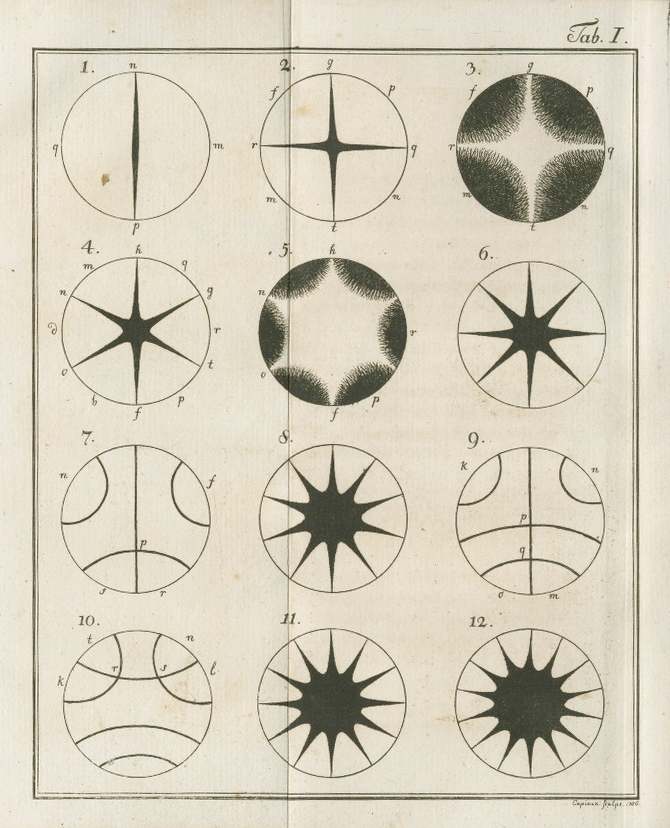
It can be easily seen from the descriptions and drawings furnished by Purkinje
[64] that all the geometric forms and designs characteristic of mescaline-induced phenomena can, under proper conditions, be entoptically observed.
Let us consider, for instance, the form constant for which "funnel," "tunnel," "cone," or similar descriptive terms are used. This form occurs again and again in mescaline hallucinations; it also appears in hypnagogic hallucinations, in entoptic phenomena, and in the phenomena arising when flickering fields are viewed under certain conditions.
Or let us consider the "honeycomb". design consisting of hexagons, Purkinje and a number of other observers saw hexagonal patterns entoptically, After awakening in the morning, Koenig
[38] frequently noticed, with eyes closed, that his whole visual field was filled up with hexagons (as in a honeycomb). The author saw after awakening, on two different occasions, a pattern almost identical with Konig's but saw it on the ceiling, and not with closed eyes.
One of Klien's
[31] patients frequently, saw, with eyes open, a hexagonal network during migraine attacks. Weil
[84] reported that he saw Konig's design when observing visual phenomena in the hypoglycemic state. The subjects of Haack
[23] saw hexagonal patterns when viewing flickering fields.
It is clear, therefore, that the honeycomb design, with its hexagonal elements, appears not only in the hallucinatory phenomena produced by mescaline but also under many other conditions. The same is true with respect to the other form constants. In an
Enquiry into the Causes of Mescal Visions Marshall
[50] has tried to show that the form constants proposed by the author can arise only from some peripheral stimulation that is common to different persons. He accounts for the different form constants by reference to various structures within the eye.
It is of special interest that among these he includes retroretinal structures and the choriocapillary circulation. He concludes from anatomical, physiological, and observational data of various kinds that “the rods and foveal cones can look backwards” and that the retinal pigment and the choriocapillary circulation can, therefore, be seen under certain conditions.
Similarly, physiologists have attempted to account for entoptic phenomena in general by connecting them with secretions on the cornea, moving particles in the vitreous humor, the network of retinal vessels, the properties and states of the cornea, lens, or other intraocular structures
[10, 49]. Hoppe
[26], one of the chief exponents of a peripheral theory of visual hallucinations, maintained as early as 1887 that “central direct, immediate, psychic) hallucinations” arising somewhere in the brain do not exist and that “the entoptic content of the eye” always furnishes the “hallucinatory material.”
Morgenthaler
[55] and others have emphasized peripheral factors even in the hallucinations of dementia praecox patients. Zucker
[90] injected mescaline into patients who had hallucinations. As a result of these injections, the tapestry design and modifications of the chessboard design appeared, among other hallucinatory phenomena, in some of his schizophrenic patients.
Zador’s patients with tract hemianopia (amaurosis of one eye, blindness in temporal region of other eye) saw, under the influence of mescaline, kaleidoscopic phenomena, squares, and other geometric figures in the whole visual field before both eyes
[88].
A totally blind patient (amaurosis due to tabes) frequently reported seeing a beautiful chessboard design in the mescalinized state, but he also saw a blue pattern with regularly distributed white points when he was not under the influence of the drug. Mescaline did not induce any visual phenomena in a 23-year-old patient whose eyes had been enucleated during the second year of life.
It must be said that the experiments on patients with some pathology of the visual system leave so many points unsettled that no general conclusions are warranted. The visual effects, as well as the conditions under which they have been obtained, are often so incompletely described that even available data cannot be interpreted.
As Guttmann
[21] has pointed out, the crucial experiment with congenitally blind persons still remains to be done. It is a well-known fact that blind persons often report subjective visual Phenomena, such as scintillation or photopsiae like “flames or “sparks,” but sometimes they also report definite forms and figures, Whether these figures ever show the patterning indicated in the various form constants described has not yet been systematically investigated.
Clear-cut results as to the form constants present in the visual. experiences of persons with loss of both eyes or totally blind for other reasons, examined at different intervals after the onset of blindness, are not available. One of the author's blind subjects (enucleation of left eye, glaucoma of right eye) saw "halts with oval shape," either still or moving, appearing before him at a distance of about 5 feet. The halls wept about as large as a dime and were only occasionally colored. chiefly red or violet.
He also reported seeing "silver bars," 'arabesques," "rings into which you can put your finger," and "shiny test tubes." He claimed that the phenomena were More prominent before his left eye, which had been removed 1.5 years ago, and that they did not appear at all on certain days. it was impossible to elicit more definite information.
Alternating current did not influence or banish these phenomena. The nicker phenomena that are been by normal subjects under certain conditions of stimulation with alternating current
[65] could not be electrically produced in this subject. It should be mentioned that the 'form' constants that we have discussed arc apparently not typical for the visual phenomena produced by electrical stimulation of the occipital lobe in man.
Urban
[78] found that the photopsiae consisted mostly of glowing and colored "roundish forms, disks, or rings" when Faradic current was used and of stars and ragged forms such as "pointed sparks" when galvanic current was used.
It should be obvious that the factors determining the appearance of certain form constants are so numerous that all theories stressing either 'peripheral' or 'central' factors are too simple. That there is an interaction of these factors may be true, but this remains in the present state of our knowledge a vague assertion.
We wish to stress merely one point, namely, that under diverse conditions the visual system responds in terms of a limited number of form constants. Any general theory. however, will have to beyond a consideration of visual mechanisms per se. The mescaline-produced phenomena demonstrate this point in a striking manner. Mescaline induces changes not only in the visual field but also in other sensory spheres, particularly in the sornatosensory sphere.
Haptic hallucinations — and other somatosensory phenomena may dominate the symptomatology to the exclusion of phenomena in the visual sphere. We shall not enter into a description of the somatosensory changes, but merely mention that Professor Forster
[16], for example. felt a net similar to a "cobweb" on his tongue: "When 1 opened my mouth, a cold wind passed through and the net moved." Serko
[72] frequently had the sensation that his legs or his Feet consisted of "spirals." In his case, sometimes the haptic spiral of a leg blended with a luminous spiral that had been rotating in the visual Field: "One has tile sensation of sirimatic and optic unity."
To dismiss such phenomena as synesthetic-experiences merely emphasizes the present lack of knowledge concerning the processes involved in synesthesias and intersensory relations in general. A physician, a subject of Beringer
[4], "saw and felt" the sounds of li concertina. played by the experimenter, and the pain produced by it coagulated as luminous curves in the spiral turns of his body, the lower part of his body being a grren varnished time with spiral windings.
Such experiences would probably be classified as instances of complex synesthesias, However. a form constant may involve so many spheres that even a synesthetic basis would be too narrow. In one of Beringer's subjects (also a physician), the "lattice" or "fretwork" constant became so dominant that it appeared in penetrate the whole personality.
The subject stated that he saw fretwork before his eyes. that his arms. hands. and fingers turned into fretwork aml that he became identical with die fretwork. There was no difference between the fretwork and himself; between inside and outside. All objects in the room and walls changed into fretwork and thus became identical with him. While writing, the words turned into fretwork and there was, therefore, an identity of fretwork and handwriting. "The fretwork is I". All ideas turned into glass-fretwork, which he saw, thought, and felt. He also felt sore, tasted and smelled tones that became fretwork. He himself was the tone. On the day following the experiment, there was Nissl (whom he had known in 1914) sitting somewhere in the air, and Nissl was fretwork. "I saw him, I felt him; Nissl was I."
It seems necessary to assume some basic process operative in diderent sense modalities to cope with all varieties of synesthetic triperiences. Even the fact that a sensory impression or a hallucination in one of the sense fields is followed by 'manifestations in tither sense fields does not give us the right to speak of "primary" ind "secondary" sensations (or hallucinations) except in the case of temporal succession.
One event may be primary and another secondary in this sense, and yet the intersensory relation may involve only one basic process. Similarly, we may doubt whether the preceding example of a "mescal psychosis" with "fretwork" or 'lattice" as the central theme can be understood by considering the hallucinatory occurrence of the fretwork in the visual field a "primary" event that determines "secondary" and "tertiary," etc., events such as changes in other sense fields and in the mechanism of thought and emotion.
In a further search for hallucinatory constants, we shall again start with a consideration of the form factor. We note that a single form (figure, object) may be duplicated or multiplied, that its size may change or that its shape may be altered or distorted; i.e, we may have monocular or binocular diplopia or polyopia; dysmegalopsia (micropsia or macropsia); metamorphopsia or dysmorphopsia. If we analyze the visual phenomena produced by mescaline, we find diplopia, polyopia, tlysmegalopsia, anti dysmorphopsia not only of hallucinatory objects but also of real or imaginal objects. That is to say. the same mechanisms may be operative, no matter whether an object is perceived, imagined, or hallucinated.
The mescaline experiments demonstrate, therefore, that we must go beyond the level of visual hallucinations to determine hallucinatory constants. In fact, we must even go beyond the visual mechanisms that cut across distinctions between perception, imagery, and hallucination and raise the question whether similar mechanisms are operative in nonvisual spheres. There is no doubt that polyopia, dysmegalopsia, and dysrnorphopsia find their parallel in experiences in the somatosensory sphere. Subjects in the mescalinized state feel that their limbs shrink or grow, that they are shortened or elongated, or that they are distorted in many ways.
The experience of changes in size and the sensation of distortions anti alterations may involve the whole body. As regards polyopia, its counterpart is found, for example, in a "polyrnelia" of the fingers or of the arms. The subject may feel several arms growing out of his shoulder until be feels "like the Buddhas." At times, the alterations in the somatosensory sphere may be so profound that parts of the body feel separated from the rest. As Serko insisted, there may be, not a "sensation" but a "somatopsychic hallucination" of two bodily forms, e.g., of an amputated leg and of a foot entirely separate lying beside it.
The tendency toward reduplication appears not only in polyopia and "polyrnelia" but also in hallucinatory experiences involving the presence of one or many persons in the room. Although these persons are not seen, their reality is in some way experienced or "felt." ln this connection, it is of interest that "splitting" of personality and various degrees of "depersonalization" have been frequently reported.
It may be said, therefore, that polyopia, dysmegalopsia, and dysmorphopsia involve mechanisms that are characteristic of mescaline-induced phenomena not only in the visual sphere (hallucination, imagery, perception) but also in the sornatosensory sphere. Further analysis reveals the fact that mescaline is only one of many agents bringing about polyopia, dysmegalopsia, and dysmorphopsia. Thus, under certain conditions, the same effects can be observed in psychogenic and non-psychogenic hallucinations, even in the
hallucinations autoscopiques, in the perception of real objects; in visual imagery; in dreams; in eidetic imagery; in hypnagogic hallucinations; in the phenomena that arise when flickering fields are viewed
[4, 12, 14, 15, 23-25, 2-9, 36, 51, 53„ 58, 66, 69, 83, 84].
In other words, reduplication or changes in size or shape of a given visual form may occur, no matter whether the object in question is real or has appeared as the result or looking for a considerable time at a flickering field — whether it is hallucinated, visually imagined, or seen as an eidetic or hypnagogic image. In fact, some spontaneous drawings seem to exhibit similar tendencies, so that Maclay, Guttmann, and Mayer-Gross speak of a "mescaline 'type" of drawing.
[45]
By way of summary, it may be said that polyopia, dysmegalopsia, and dysmorphopsia occur not only in visual hallucinations but also in many other phenomena of the visual sphere (visual perception, eidetic imagery, dreams, etc.). The fact that diverse visual phenomena commonly assigned to different functional levels of the visual system may show the same lyrical behavior becomes of still greater interest if we consider the various conditions and clinical states in which such typical behavior occurs.
The "symptoms" of polyelpia, dysmegalopsia, and dysmorphopsia have been observed in different psychoses, especially in toxic psychoses or at the beginning of certain psychoses; in delirums; in insulin hypoglycemia; in hysteria; in patients with urrebral lesions (particularly with parieto-occipital or occipital) lesions in the basedoid constitution, in eidetic individuals, and in posionings produced by certain drugs (hashish, cocaine, etc., chronically used).
Beringer
[4] has called attention to the existence of these symptoms in the acute phases of schizophrenia, The symptoms were especially striking in one of his hebephrenic patients. Gurewitsch
[18, 19] has described an "interparietal syndrome" in which polyopia, dysmegalopsia, and dysmorphopsia are combined with alterations in the postural model of the body or in the bodily schema (head). According to him, this syndrome is found in nosologically different diseases, such as
lues cerebri epilepsy, schizophrenia, hysteria, and cerebral trauma.
Thus, the optical symptoms paralleled in the somato-psychic sphere in other conditions as well as in mescaline intoxication. In trying to account for polyopia, dysmcgalopsia, and dysphopsia, ophthalmologists have stressed the importance of dioptric and retinal conditions. Such conditions, however, are not enough to explain the occurrence of similar visual changes in imaginal objects or the fact that the alterations selectively affect only specific objects in a room or only parts of certain objects.
Since the optical symptoms occur under many different conditions and in diseases with different etiology, the relative importance of the various factors influencing the visual mechanisms may be expected to vary in different conditions or from one disease to the other, However, we should not necessarily expect entirely different factors to become operative, if polyopia and related symptoms appear in a schizophrenic; a mescalinized or eidetic individual; or in a patient with a parieto-occipital lesion.
The search for some basic factor underlying the optical symptoms in etiologically different conditions is undoubtedly surrounded by the same difficulties as the search for so-called neurological syndromes in psychoses. The "interparietal syndrome" of Gurewitsch is present, for instance, not only in patients with cerebral lesions but also in schizophrenic patients in whom such lesions are absent. It would be rash to conclude that the same syndrome is produced by two different agents. Unfortunately, we are far from knowing the pathophysiological mechanisms that become operative as the result of a parieto-occipital lesion.
Once the nature of these mechanisms is known, we shall perhaps understand why the same symptoms mar appear, for instance, in schizophrenic patients. The diversity of conditions in which polyopia, dysmegaiopsia, and dysmorphopsia occur has not deterred investigators from looking for some fundamental mechanism. That such a mechanism must be assumed is strongly suggested by the fact that polyopia and related symptoms are characteristic not only CIF different functional levels in the visual sphere (perceptinn, imagery, halludnation, etc.) but also of the somatosensory sphere.
In recent years, the analysis of these symptoms has led most investigators to assign a fundamental role to vestibular factors. ft is thought that reduplication of objects, micropsia., macropsia, and dysmorphopsia. in hallucinations are indicative of a vestibular influence. The same conclusion is reached, for example, by Menninger-Lerchenthal
[53] in his thoroughgoing analysis of autoscopic hallucinations. His view is that autoscopy is a hallucination of the bodily schema which has a visual and a tactile-kinesthetic component. He believes that it does not make any difference whether the study of autoscopic hallucinations is approached from the phenomenological angle or from facts of brain physioiogy, since the analysis always leads to vestibular factors. Skworzoff
[74] has presented similar views.
Other investigators have emphasized tonic, postural, and oculomotor factors. In this connection, it is of interest that Poetzl and Urban
[6] have stressed the importance of the supravestibular, system (in the sense. of Muskens). The experimental data on the influence of the vestibular aparatus on the visual sphere are rather meager.
Most of the experiments have been concerned with determining the effects of various forms of labyrinthine stimulation (rotation, galvanic, or caloric stimulation) on different visual phenomena. There is no doubt however, that the available anatomical, clinical, and experimental data are sufficient for supporting the view that any future research directed toward elucidating the role of the vestibular system is bound to yield extremely significant results not only for the study of hallucinations but also, as some neurologists and psychiatrists insist, for a deeper understanding of neurotic and psychotic behavior.
It has even been maintained, particularly by French neurologists, that great strides will be made in psychiatry by obtaining data on vestibular chronaxy. At this point, it is not possible to outline the various experimental problems that urgently require a solution. We shall be content with calling attention to a new technique that may be employed in analyzing different factors influencing hallucinations or other subjective visual phenomena.
By applying alternating current of low intensity and frequency, it is possible to produce flicker that is visible with open or closed eyes under conditions of light as well as dark adaptation. During recent years, the author has obtained some data on the behavior of negative after-images, eidetic images, and hallucinations in the presence of electrically produced flicker.
For evaluating the flicker phenomenon itself, it was necessary to examine patients with some pathology of the visual system (hemianopia, enucleation of one eye, ctc.). In general, negative after-images disappear almost entirely or change radically in appearance the moment the stimulating current is turned on.
Cessation of electrical stimulation immediately leads to a reappearance of the after-image and to a restoration of its normal properties, Eidetic images and certain types of hallucinations may vanish, change, or remain unaltered upon appearance of the electrically produced flicker.
To illustrate: one subject, a student, saw an eidetic image of the face of a person looking at him, When the current was turned on, he suddenly saw the profiles of five faces looking to the right. These faces rapidly changed into other faces; they were seen through the “muslin curtain” of the flicker, as the subject ex- pressed it. More than three decades ago, Urbantschitsch
[79, 80] used galvanic current for influencing eidetic images.
He reports eg. that one of his subjects saw an eidetic image of a hepatica. Application of the galvanic current immediately led to | the appearance of a large number of hepaticas. It should be realized, of course, that rotation of the subject, or electrical and other forms of stimulation, may merely accentuate tendencies inherent in specific objects in a row or only parts of certain objects, since the optical symptoms occur under many different conditions and in diseases with different etiology, the relative importance of the various factors influencing the visual mechanisms may be expected to vary in different conditions or from one disease to the other.
However, we should not necessarily expect entirely different factors to become operative if polyopia and related symptoms appear in a schitzophrenic, a mescalinized or eidetic individual or in a patient with a parieto-occipital lesion. The search for some basic factor underlying the optical symptoms in etiologically different conditions is undoubtedly surrounded by the same difficulties as the search for so-called neurological syndromes in psychoses.
The "interparietal syndrome" of Gurewitsch is present, for instance, not only in patients with cerebral lesions but also in schizophrenic patients in whom such lesions are absent. it would be rash to conclude that the same syndrome is produced by two different agents.
Unfortunately, we are far from knowing the paraphysiological mechanisms that become operative as the result of a para-occipital lesion. Once the nature of these mechanisms is known, we shall perhaps understand why the same symptoms may appear, for instance, in schizophrenic patients. The diversity of conditions in which polyopia, dysruegalopsia, and dysmorphopsia occur has not deterred investigators from looking for some fundamental mechanism.
That such a mechanism must be assumed is strongly suggested by the fact that polyopia and related symptoms are characteristic not only of different functional levels in the visual sphere (perception. imagery, hallucination, etc.) but also of the somatosensory sphere. In recent years, the analysis of these symptoms has led most investigators to assign a fundamernal role to vestibular factors. It is thought that reduplication of objects, micropsia, macropsia, and dysmorphopsia in hallucinations are indicative of a vestibular influence.
The same conclusion is reached, for example, by Menninger, Lerchenthal
[53] in his thoroughgoing analysis of autoscopic hallncinatinns. His view is that autoscopy is a hallucination of the bodily schema which has a visual and a tactile kinesthetic component. He believes that it does not make any difference whether the study of limoscopic hallucinations is approached from the phenomenological angle or from facts of brain physiology, since the analysis always leads to vestibular factors. Skworzoff
[74] has presented similar views.
Other investigators have emphasized tonic. postural, and octillomotor factors. In this connection, it is of interest that Poetzl and Urban
[63] have stressed the importance of the supravestibular system (in the sense of Muskens).
The experimental data on the influence of the vestibular apparatus on the visual sphere are rather meagre. Most of the experiments have been concerned with determining the effects or various forms of labyrinthine stimulation (rotation, galvanic, caloric stimulation) on different visual phenomena.
There is doubt however, that the available anatomical, clinical, and experimental data are sufficient for supporting the view that any future research directed toward elucidating the role of the vestibular system is bound to yield extremely significant results not only for the study of hallucinations but also, as some neurologists and psychiatrists insist, for a deeper understanding of neurotic and psychotic behavior.
It has even been maintained, particuarly by French neurologists, that great strides will be made in psychiatry by obtaining data on vestibular chronaxy. At this paint, it is not possible to outline the various experimental problems that urgently require a siolution. We shall be content with calling attention to a new technique that may be employed in analyzing different factors influencing hallucinations or other subjective visual phenomena.
By applying a current of low intensity anti frequency, it is possible to produce flicker that is visible with open or closed eyes under conditions of light as well as dark adaptation. During recent year the author has obtained some data on the behavior of negative after-images eidetic images, and hallucinations in the presence of electrically-produced flicker. For evaluating the flicker phenomenon itself. It was necessary to examine patients with some pathology of the visual system (iemianopia, enuelcation Of one eye, etc.).
In general, negative after-images disappear almost entirely dissapear in appearance the moment the stimulating current is turned on. Cessation of electrical stimulation immediately leads a re-appearance of the after-image and to a restoration of its noival properties. Eidetic images and certain types of hallucinations may vanish, change, or remain unaltered upon appearance of the elmtrically produced flicker.
To illustrate: one subject, a student, saw an eidetic image of a face of a person looking at him. When the crrent was turned on, he suddenly saw the profiles of five faces looking to the right. These faces rapidly changed into other faces; they were seen through the "muslin curtain" of the flicker, as the subject expresssed it.
More than three decades ago. Urbantschitsch
[79, 80] used galvanic current for influencing eidetic images. He reports eg. that one of his subjects saw an eidetic image of a hepatica. Application of the galvanic current immediately led to the appearance of a large number of hepaticas.
It should be realized, of course, that rotation of the subject or electrical and other forms of stimulation may merely accentuate tendencies inherent in eidetic. In an attempt to define hallucinatory constants, we have purposely taken visual forms and their interrelations as a point of 'departure.
It is obvious that we have ignored many aspct of hallucinatory phenomena in order to arrive at these conclusions. The hallucinatory constants that we have found may be tentatively assigned assigned to three levels:
- The level of "form constants".
- The level of alterations in form, size, and shape. (polyopia, dysmegalopsia and dysmorphopsia.
- The level of changes in spatio-temporal realations.
We have shown that the same constants appear in other visual, and even in nonvisual, phenomena. These constants are, therefore. riot specific for hallucinations but represent general characteristics. The "structure" of hallucinations is a general structure that is typical of numerous phenomena in the visual sphere.
THE CONTENT OF HALLUCINATIONS
Since we have been interested in an analysis in terms of formal criteria, we have paid no attention to the content of the hallucination. If a childless woman hallucinates many babies, it is readily assumed that the hallucination represents a
projection of affective needs. But if it should be found that the same woman, when looking at a pencil or a chair, suddenly sees a row of pencils or a row of chairs, it appears unlikely that emotional factors are responsible for the multiple seeing of objects.
Of course, any object, no matter whether it is eidetically seen, hallucinated; imagined; or perceived as a real object, may be of emotional significance. It is one thing to admit that objects in multiple vision may have emotional significance: it is an entirely different thing to asiert that polyopia it is created by emotional factors.
One of Schilder's
[67] patients, an officer with a crippled arm, saw in a fever delirium all persons around him with crippled or missing arms and legs. A blind patient hallucinated heads with empty eye-sockets. Following an ophthalmological examination, a schizophrenic woman stated that one of her eyes was red and inflamed. Subsequently she saw all persons in the room with one red eye
[63].
It may be said that, in such cases of transitivism, to use Wernicke's expression: Affective factors determine the content of the hallucination. However, to say that the projection of disturbances is the motor, vaso-motor, and cenesthetic spheres, or of other disturhances, occurs on an effective basis is an empty statement and acids nothing to our knowledge about the workings of affective mechanisms.
We want to know the exact nature of these mechanisms in a given case. We seek to know why a particular object should appear. In a hallucination under the stress of some affective need is not more surprising than the fact that the perception of objects, even of a Mark line, may be 'modified' by affective factors.
Psychologically, objects per-se have no existence: they exist only nodal points in a network of perceptual, affective, or logical relations. It is the determination of these relations that is the task in psychology. A live bull snake; a boa constrictor; a motion picture; and a wavy black line of certain dimensions may lead to relations of fear in a certain monkey, whereas a live garter snake and a boa constrictor in a film running at a higher speed may not.
It is not a certain site, color, shape, or speed of movement that causes to the manifestation of fear in the monkey but a specific sense of 'togetherness' of these properties that constitutes the behaviorally effective stimulus, and this can be determined only experimentally.
We cannot specify the psychological nature of the "fear" existing in the animal without specifying the effective stimulus properties existing outside the animal. Certain objects or events become emotionally equivalent because they share certain properties. By studying the properties of equivalent and non-equivalent situations, we may be able to learn something about the nature of the affective mechanism. Under the influence of different affective factors, objects and events become imbued with different properties, just as under one set of conditions a circle becomes perceptually "similar" to and, under another set of conditions, "different" from an elipse.
The affective mechanism in a crippled patient who hallucinates the absence of a leg not only in other persons but also in their photographs and mirror images, as wel as in dogs and chairs, is undoubtedly not the same as the affective mechanism in Schilder's patient, who saw his defect only in other persons.
As far as dreams are concerned, a widely held theory explains their content by reference to affective factors. It is assumed that all dreams are wish fulfil ments. According to this theory, the appearance of certain objects and events in a dream is determined by some egocentric wish. Certain considerations are pertinent here.
Objects and events, no matter whether they exist in the external world, in a hallucination, or in a dream, may be similar and dissimilar in many respects. To understand particular forms of similarity, we have recourse to mechanisms of sensory organization, to affective factors, to logical relations, etc. The author previously pointed out
[37] that it is by virtue of certain similarities that heterogeneous objects and events lie in the same "dimension" or belong to the same "series" and that the problem of determining basic mechanisms in animal and human behavior often reduces itself, therefore, to determining and locating properties or factors in terms of which diverse objects and events may become similar.
It may be said that the behavioral reactions of animals as wel as the perceptual and affective reactions or processes of "abstraction" in man proceed by constantly shifting "dimensions," i.e., by constantly destroying similarities and constantly creating new ones. The existence of similarities presents, therefore, no problem; the only problem consists in determining just why particular similarities exist. The occurrence of similarities, i.e., the fact that there exist certain characteristics, factors, or processes that bind objects together and relate them in many specific ways, seems to be of such fundamental nature that the physiologist, Kries, considered it simply an expression of some basic property in the functioning of the central nervous system.
Freud, for instance, was forced to the conclusion that the factor of similarity is of paramount importance in the mechanism of dream formation. Since the fundamental role of similarity is apparent in any other group of psychological phenomena, it is not surprising that any superficial analysis of dreams leads to the same result. However, we must demand that the analysis of the phenomena provides us with the particular factors that account for the specific ways in which objects and events are related. To account for particular similarities, factors ranging from physical Gestalten to castration complexes have been advanced.
It is not the large range of such factors that presents a serious problem; the chief difficulty lies in determining which particular factor accounts adequately for certain relations between objects and events, whether it is, for instance, "visual asymmetry" or "fear of bodily injury."
We recall that in eidetic images and certain other phenomena we find translocation of objects or transfer of certain characteristics of these objects, fusions and composite formations, substitutions, the appearance of parts instead of wholes, the nonappearance or the belated appearance of objects or parts of objects, reversals of right and left, up and down, or of other directions. In other words, we find condensation, displacement, and other mechanisms that have been considered typical of dream formation.
In eidetic individuals, similar changes may occasionally appear in the perception of real objects and thus become more easily amenable to an experimental approach. From various studies, it is evident that phenomenal properties of objects, visuo-spatial factors, and motor factors play a great role in effecting condensations, displacements, and similar changes in eidetic imagery.
This suggests the possibility that the changes in dreams, such as condensations and displacements, frequently result from an operation of the same (visuo-spatial, motor, etc.) factors. In eidetic images, some of these changes can be experimentally demonstrated by setting up certain conditions. The fact that colors, shapes, movements, etc., occur at al in eidetic images, dreams and related phenomena can be understood only by reference to some fundamental properties and processes in the visual system; it seems that the occurrence of certain condensations and displacements can be accounted for only on a similar basis. It should also be recalled that G. E. Müller went so far as to consider the behavior of the eidetic images studied by Urbantschitsch as an example of the influence of "apsychonomic" (anatomico-physiological or metabolic) factors.
Urbantschitsch was able to produce a variety of changes in eidetic images by a compression of blood vessels or by the application of visual, auditory, thermal, and other stimuli. At any rate, if visuo-spatial factors lead, for instance, to the fusion of several houses or persons into one, the condensation itself is obviously not created by some affective reaction toward nudity or some similar factor, although, once created, it may stil serve as a vehicle for affective needs.
To understand the occurrence of certain spatio-temporal changes in visual phenomena, we must have recourse not only to such factors as brightness, color, shape, and spatial organization but also to factors by virtue of which colors and geometric figures, colors and melodies, sounds and lines may become similar and belong to the same "dimension."
Recently, it has even become necessary to resort to "physiognomic characters" to account, for instance, for the similarity between a handwriting, a painting, and the gait of a person. We merely wish to emphasize that the operation of visual factors alone may lead to reversals, displacements, condensations, etc. This does not mean that numerous other factors may not play a role. In an experimental study, Pötzl
[62] found that the development of dreams was determined by visual, motor, and "symbolical" factors and that the first two factors were "relatively independent of psychoanalytical factors." He believes that "repressed psychic material," being itself Gestalt-less, may act like a catalyzer for optical and motor processes.
Whether the psychic material is "repressed" or not does not concern us here, but it is obvious that any color, shape, movement, reversal, displacement, condensation, etc., once supplied by visual or motor processes, may become imbued with "meaning" and that "meaning," in turn, may guide visual and motor reactions.
There is no question that all these factors are also operative in the visual perception of the outer world, but the spatiotemporal stability of external objects is such that fusions, displacements, and the like do not occur in general. Dreams, it has been said, are similar to "eidetic images of the basedoid type." They seem at least similar in that the visual "stuff" they are made of is more open to an invasion of psychic factors than the "stuff" of other visual phenomena.
The visual "stuff" provided by entoptic phenomena, flickering fields, ink blots, dreams, eidetic images of the basedoid type, pseudo-hal ucinations, and certain types of hallucinations is apparently more easily invaded by psychic factors than the "stuff" furnished by the perception of real objects, after-images, eidetic images of the tetanoid type, mescaline hallucinations, and certain other types of hal ucinations. It is for this reason that phenomena of the first type have frequently been utilized to learn something about the deeper layers of "personality."
If, for physiological reasons, sleep should suddenly provide us with phenomena of Sinnengedächtnis or belated after-images instead of dreams, even "repressed" wishes would not succeed in changing and distorting the visual material. At this point, attention should be called to certain facts that may prove to be of interest in connection with physiological or psychological studies of dreams. Since, in most dreams, visual elements are dominant and since striking alterations in the visual sphere are characteristic of mescaline effects, it seems reasonable to expect an enhancement of dream phenomena under the influence of mescaline.
An analysis of available data, however, indicates that most subjects report an absence of dreams for the night fol owing the intoxication, and others refer only to "ordinary dreams." Even though the night may have been dreamless, the next day often provides evidence that the visual system has not yet returned to its normal state. In the literature, the author found only one reference to "unusually plastic, colorful dreams," the nature of which was not described
[4].
It seems, therefore, that, contrary to our expectations, mescaline does not lead to all enhancement of dreams and that it may even suppress dream activity. This can be only a tentative conclusion, since the whole problem has not been systematical y investigated. We know nothing about the effects in chronic mescalinism. Ludlow
[43], who has given the most detailed account of the effects of chronic hashish intoxication, points out that his rest was absolutely dreamless during time whole progress of his hashish life, whereas "he never slept without some dream, more or less vivid" before acquiring the habit.
The visions of the drug entirely supplanted those of nature." Further research should explore the mechanisms of drugs which, under certain conditions, produce striking visual effects in the waking state and at the same time do not increase or even suppress dreams, i.e., that are primarily visual in nature. In contrast to mescaline and hashish, drugs such as alcohol may turn sleep into a sommeil vigile that is constantly interrupted and haunted by extremely vivid dreams ("200 dreams in a night").
According to Epstein
[13], such effects are particularly characteristic of the pre-psychotic phases of alcoholic psychoses. This author even speaks of a "hypnagogic form of alcoholic insanity," since the long-lasting and colorful hypnagogic images in such alcoholics become frequently the starting point for various delusions.
The self-observations of the writer confirm the impression gained from the literature that the night following the mescaline intoxication is either dreamless or practical y devoid of visual dream elements. In one of the author's experiments, he saw, on awakening in the morning after a dreamless night, that the kaleidoscopic play of mescaline patterns was stil present. The patterns were predominantly violet and could be seen with open or closed eyes. He fell asleep again.
During this period of sleep lie had a dream that may be properly called a "mescaline" dream:
I am lying in bed in a large hall. It seems to me that there are many similar beds in this hal which are also occupied. I turn over to my right side and see a large window which I subject to close inspection. I see clearly the following black letters R E S T A U R. It surprises me that I can even distinguish letters. To the right of time last R is a vertical pipe, and I am aware of the fact that it covers additional letters. In the window is a large bottle containing red liquid. There are three words on this bottle. These words are complete and meaningful; yet I am dissatisfied with the third word, because I feel that it is somehow too short.
The words are surrounded by a reticulated pattern in delicate greenish colors giving the effect of a decorative label. The scene sudddenly shifts, and I find myself looking at time gray wall of a house. Very delicate fragile objects resembling unshel ed peanuts are regularly distributed over time whole surface, thus forming a lattice-like pattern.
Each husk stands on end, forming an angle of approximately 45 degrees with the surface of time wall. Violet clouds pass across the surface. This makes me wonder whether the whole phenomenon is merely a hallucination. To determine whether such is the case I close my eyes; but I stil see violet clouds. I conclude that the house and the peanut lattice have objective existence and that the violet clouds are of hallucinatory origin.
At this point, we cannot undertake analysis of this dream with reference to mescaline phenomena in general and the phenomena experienced on the preceding day or consider it in the light of other psychological factors. We merely wish to state that the mescaline structure of this dream is fairly obvious and that its mescaline-determined elements range from presque vu experiences
[33] to mescaline patterns on objects.
In studying hallucinatory and related phenomena in time visual field, we find that they are interrelated in many ways, not only in terms of certain "constants" but also in the sense that the same content is experienced on different levels or that a transformation in content is accompanied by a transition from one level to another. It is, of course, wel known that the same content may again and again appear on the same visual level, e.g., in an eidetic image, in a hallucination, or in a dream, etc.
An eidetic subject may always see the same red cap or the same house when he closes his eyes. One of Ewald's patients
[14] saw in three different deliriums the same three huge brown dogs with blue eyes entering his room, except that the third time they suddenly opened their mouths and said, "But this time it's real y we." In contrast, we have the appearance of the same content on different visual levels, e.g., when a visual scene experienced in a fever delirium in childhood reappears several decades later in a mescaline hal ucination. Guttmann
[20] describes a mescaline hallucination that reappeared as a hypnagogic image 2 years later, when one evening he fel asleep after an exhausting day during the First World War. He recognized the identity of the content only when he studied old protocols 5 years afterward. It has also been reported that the content of a hypnagogic image may reappear in a dream. A mescaline hallucination may be the reproduction of a previously perceived visual object, such as a geographical map. In the experience of the individual, a visual memory-image may transform itself into an eidetic image; a positive or negative after- image, into a mescaline hallucination; and a pseudohallucination, into a hallucination.
"HALLUCINATIONS" VS. "SYNDROMES WITH HALLUCINATORY ELEMENTS"
Although it may be true that the complexity of visual hallucinations and related phenomena is somewhat reduced by an analysis which shows that the same constants or even the same contents appear on different visual levels, it does not alter the fact that there stil remain many phenomenal characteristics and forms of behavior in hallucinations, eidetic images, dreams, etc., which are refractory to such an analysis.
For example, if we consider the phenomenology of mescaline-induced hallucinations, we find "primitive" as wel as "scenic" or "panoramic" hal ucinations or, expressed differently, mescaline-specific" and "mescaline-nonspecific" hallucinations
[91]. It should be remarked that our analysis has been largely confined to "primitive" or "mescaline-specific" hallucinations. Furthermore, it is clear that the total picture of primitive" and "scenic" mescaline hal ucinations is related to changes in other sense fields anti ultimately can be understood only by also considering alterations affecting the total personality. We are undoubtedly safe in assuming that the hallucinatory phenomena in a mescalinized person dictating a description of his visual experiences to an assistant are in some way not the same as those of a person in a "mescal psychosis."
Kinnier Wilson
[85], for instance, refers to an individual who, under the influence of mescaline, was found "crawling about the floor with extreme care, but averred he was a fly walking on the ceiling upside clown and that if he moved quickly he would fall and be injured." In applying the term hallucination to phenomenologically anti genetical y different phenomena, most investigators have tacitly assumed that they are dealing with the "same' symptom and that criteria employed in studying, for instance, visual hal ucinations are also applicable to hallucinations in other fields.
However, an "hallucination" always appears as an element in a complex of other symptoms. Schröder
[71] doubts, therefore, that there is such a thing as a "hallucination," i.e., something which, as an elementary symptom, can be detached from other symptoms and independently studied by comparing it, for instance, with "hallucinations" in other sense fields. He insists that only the whole complex of symptoms, in which tile hal ucinations appear, can be profitably studied and describes four such "complexes with hallucinatory elements": (a) deliriums; (b) verbal hallucinosis; (c) sensory deceptions associated with affective states (anxiety, delusions of reference); (d) hal ucinosis phantastica (paraphrenia). He questions the sensory basis of many so-called sensory deceptions.
It is apparent from a study of the literature that ever-renewed efforts have been made to evolve criteria suitable for describing and classifying the whole range of hallucinatory phenomena. The literature has grown to such proportions that Mourgue
[57], for instance, found it necessary to consult more than 7000 titles. In an attempt to cope with the wealth of subjective phenomena arising under normal and pathological conditions, investigators have considered such factors as levels of reality, states of consciousness (degree of "clouding"), phenomenal appearance, the relation to "inner" and "outer" space, and the relation to "intentions" or "acts" of the subject.
The employment of such criteria has led to a classification of the phenomena into hallucinations, pseudohallucinations, il usions, eidetic images, eidetic images with Realitäts-charakter, hypnagogic images, reperceptions, Sinnengedächtnis, memory-after-images, pseudo-memory-images, and phantastic visual phenomena. This does not exhaust the number of distinctions drawn on various grounds. For example, hallucinations have been divided into "psychogenic" anti "nonpsychogenic," eigentliche and uneigentliche, positive and negative hallucinations.
In view of the large number of distinctions available, we should expect that an investigator would have no difficulty in assigning the various sensory deceptions in his subjects or other forms of subjective experiences their proper place in a classification of hallucinatory and related phenomena. However, this is far from being the case. The first difficulty arises from the fact that in actual experience there are many transitions and transformations, so that, for example, an il usion or a hynagogic image may turn into an hallucination.
A second difficulty is more serious. It frequently happens that the hal ucinatory experience of the subject is such that it cannot be adequately described and classified in terms of available concepts. Klein
[30], for instance, found that current definitions were of no use in characterizing the hemianopic hallucinations of his patients and that these could be described only as "special forms of pathological experience." Many other phenomena arising under normal and pathological conditions display the same resistance to being labeled and to not fit into any classificatory scheme. In the case of eidetic imagery, for instance, the question has been raised whether the experience of the subject should be classified as a projected memory-image, a pseudo-hallucination, or a hallucination
[28, 60].
A similar question arises with regard to "mescaline hallucinations." We have used the term "mescaline hallucinations," only to characterize the phenomena in a preliminary way. Even the self-observations of qualified observers have not settled the point whether the phenomena arising at certain stages of the poisoning should be designated as hal ucinations or pseudohal ucinations. Some observers hold that they are pseudohallucinations in the sense of Kandinsky; others believe that the phenomena can be described only by reference to a new concept of "pseudohal ucination" different from that of Kandinskv. Instead of classifying the phenomena, some investigators have been content with references to the state of consciousness of the subject or the level of reality on which the phenomena appear.
Claude and Ey
[7] state than an "hallucinogenic substance" such as mescaline produces an osmose du réel et de l'imaginaire. Ewald (14) thinks that we are dealing with hallucinatory-dreamlike experiences occurring in "a kind of delirium without clouding of consciousness" and reports that a similarly "rich optically delirious picture" without clouding of consciousness is sometimes found in cases of chronic encephalitis and in patients with hypophysial tumors.
The fact that present concepts in the field of hallucinations cannot do justice to the wealth of normal and pathological experiences can be remedied in only two ways. It must be recognized, first, that most categories employed in describing psychic phenomena in general are neither clearly defined nor generally agreed upon. It follows that any improvement in the conceptual tools of psychology wil benefit the study of hallucinations.
In the second place, many normal and pathological experiences have either not been analyzed so far by using techniques already available or could not be analyzed because of the difficulties of an experimental approach. It follows that new approaches and more thorough analyses wil help to define more clearly the varieties of hallucinatory experiences. Psychiatrists have recognized that many hal ucinations of dementia praecox patients are not real y hallucinations but, to use the German expression,
uneigentliche Halluzinationen.
Although the patients refer to sensory experiences of all kinds, it remains frequently obscure in what sense field the hal ucinations occur. In fact, it is questionable whether the hal ucinations really represent visual, auditory, or cenesthetic experiences or have any sensory content. It is of interest that an investigation of synesthesias in normal individuals leads into similar difficulties
[27]. It is true that an auditory stimulus may give rise to a sensation of color in some subjects, but in others the color, e.g., purple, is not actually seen. Instead, the subject experiences a "feeling like purple" or a feeling "as if purple." In these subjects it is a similarity in affective relations that is apparently responsible for the quasi-visual "as if" character of the synesthetic experience. In stil another group of subjects, the auditory stimulus calls forth merely the visual image of a color.
There are also "complex synesthesias" that are characterized by the fact that the thinking of an abstract concept (infinity, peace, sin, negation, etc.) invariably leads to seeing or imagining certain figures, or lines or to some "as if" experience of such colors, etc. The subject, for example, may have the experience of a "horizontal, sharp, thin, square plate of white metal" when thinking about "negation." We may say, therefore, that there are not only eigentliche and uneigentliche hallucinations but also eigentliche and uneigentliche forms of synesthesia.
The results of a chemical approach to these problems, however, should warn us that we cannot entirely dismiss the possibility that certain or even all "cenesthetic hallucinations" of dementia praecox patients may have some sensory basis. The profound effects of mescaline on the sensorium are known, and yet, as Mayer-Gross
[51] correctly observes, the descriptions of abnormal somatosensory experiences by mescalinized persons are often as fantastic and unintelligible as those of schizophrenics.
The third difficulty in arriving at clear concepts in the field of hallucinations arises from the complexity and inconstancy of "hallucination" as a symptom in a group of other symptoms. It is characteristic of drugs, disease processes, and other hallucinogenic factors and conditions that they produce more than one type of sensory deception. In fact, in some psychoses, there are apparently hallucinations of different types and of different sensory origin, "reflex hal ucinations," pseudo-hallucinations, illusions, and almost every kind of sensory deception ever described. Bleuler has presented a truly impressive picture of the varieties of sensory deceptions in schizophrenia.
Even in mescaline poisoning, we find different kinds of illusions, pseudo-hallucinations, and hallucinations. Furthermore, al these phenomena may be very inconstant in the sense that all or some of them may be present or absent under certain conditions or at certain stages of the disease or the poisoning. "Voices" not heard for many months may suddenly be heard again. At one time, the hallucinating may be interrupted by weak forms of external stimulation; at other times even strong stimuli are ineffective.
The fact that the same dose of mescaline may produce at different times different types of hallucinations in the same subject has led Franke
[17] to suggest serial poisonings, with intervals of days instead of months. He believes that long intervals may introduce differences in the "actual biological condition" of the individual, a condition that is undoubtedly influenced by factors such as age, hunger, thirst, fatigue, weather, nutrition, emotional states, etc.
The question may be raised, however, as to why certain psychic functions remain fairly constant and are only little affected by marked changes in the "actual biological condition," whereas hallucinatory phenomena and the hallucinatory process undergo marked fluctuations. It is of interest in this connection that similar fluctuations seem to be characteristic of the performances of patients with visual agnosia.
For example, the patient may be able to recognize certain details or general relations on one day but not on the next, or only under certain conditions; he may be able to do it spontaneously but not at wil , or vice versa. At any rate, the factors responsible for these fluctuations in hallucinatory symptoms cannot be clearly defined at present. Mourgue
[57] has advanced the view that they are due to a dysregulation of the normal relations between the vegetative system (in the sense of Kraus) and the cortex. The hal ucination, according to his view, represents an invasion of the world of "instincts" into the "sphere of orientation and causality"; it is not a "morphological" but a "secretory" disorder (in the sense of Mourgue and von Monakow) indicative of disturbances in the normal relations between the "vegetative" or "instinctive" sphere and the cortex.
Mourgue is not surprised that fluctuations and oscillations in hallucinatory symptoms represent the normal state of affairs, since the hallucination is essentially not a static phenomenon but a dynamic process, the instability of which merely reflects an instability in the conditions of its origin. Although the value of such concepts as "sphere of orientation and causality" and "sphere of instincts" for actual research may be questioned, there is no doubt about the importance of vegetative mechanisms for hunger, thirst, sex, sleep, and affective states.
Furthermore, it appears that further information on factors influencing the excitability of the vegetative system (electrolytes and lipoids, hormones, colloidal balance, etc.) wil be of far-reaching significance for the problem of hallucinations. Research in the field of hallucinations has been dominated by two chief interests. Either the investigators have been interested in the structure of the various phenomena commonly classified as "hallucinations" or they have studied the hallucination as a "symptom" in an aggregate of other symptoms. For investigative work, it matters little whether we start from the phenomenology of hallucinatory experiences or from "syndromes with hallucinatory elements," since any thorough analysis will lead to a study of many related factors.
The hallucinatory constants that we have described are characteristic not only of certain aspects of hallucinations but also of a variety of other phenomena. The existence of these constants suggests some constancy in the underlying conditions. Other aspects of hallucinations and the hallucinatory process itself are often characterized by instability and fluctuations, and it is the task of future research to deduce the occurrence of these fluctuations on the nature of the underlying mechanisms
No one would have thought a short time ago, Mourgue points out, that there ever could be any connection between tetany and the subject of hallucinations. And, we may add, no one would have thought of electrolytes and hormones in connection with hal ucinations. Ultimately we are not interested in hallucinatory constants per se but in the conditions producing them. There is no doubt that the study of these conditions wil be significant for the analysis of certain disease processes and the exploration of fundamental reaction systems in normal individuals.
The phenomenological approach finally leads to the study of certain syndromes and general reaction systems in the organism; the study of "syndromes with hal ucinatory elements" final y leads to an analysis of the hal ucinatory phenomena. Only by studying the whole complex of symptoms in mescaline intoxication, including the hallucinatory symptoms, has it become possible to recognize mescaline as an agent for the production of "experimental psychoses," and only in such a way have psychiatrists recognized the symptomatological similarity between mescaline intoxication and the acute phases of schizophrenia
[3, 4, 7, 8, 22, 47, 76]. No matter what the symptomatological relations may be, the "mescal psychosis" is produced by a wel -defined chemical substance and not by hypothetically assumed toxins, "metatoxic intermediaries," and the like.
It seems that psychotic symptoms resembling those of mescaline intoxication appear not only in the course of the schizophrenic disease process but also under other conditions. Serko
[73], for instance, described the "unusually interesting psychosis of a patient whose symptoms were strikingly similar to those produced by mescaline.
In view of these findings, it is unfortunate that at present so little is known about the biochemical processes involved in mescaline action. To complete the picture of the total effects produced by mescaline, we should mention some facts that have a more particular bearing on the study of normal and abnormal personality. It was found, for example, that posthypnotic suggestions may influence mescaline-produced hallucinations and that, in turn, posthypnotic sensory deceptions may become altered under the influence of the drug
[59].
A patient with spontaneous hemianopic hallucinations declared herself blind for the duration of the mescalinized state
[1]. A patient who had not heard "voices" for half a year heard them again while under the influence of mescaline
[89]. Other investigators have used mescaline for more frontal attacks on problems of personality. They have been interested, for example, in the reactions of different personality types, different races, and mentally subnormal individuals and in the possibility of obtaining "confessions" during the intoxication
[2, 4, 39, 47, 48, 59]. The results suggest that mescaline investigations cannot be considered the royal road to "the hinterland of character" and that the chief value of this drug lies in its effectiveness as a research tool in the solution of some fundamental problems of biological psychology and psychiatry.
REFERENCES
Reprinted in 1966, by permisson. Studies in Personality, Terman & Merrill McGraw-Hill, N.Y, 1912. pp. 175.207.
- Adler, A., & Pötzl, 0. Über eine eigenartige Reaktion auf Meskalin bei einer Kranken mit doppelseitigen Herden in der Sehsphäre. Jahrb. Psychiat. & Neurol., 1936, 53, 13-34.
- Bensheim, H. Typenunterschiede bei Meskalinversuchen. Z. ges. Neurol. Psychiat., 1929, 121, 531-543.
- Beringer, K. Experimentel e Psychosen durch Mescalin. Z. ges. Neurol. Psychiat., 1923, 84, 426433.
- Beringer, K. Der Meskalinrausch. Monogr. Gesamtgeb. Neural. & Psychiat., 1927, 49, 1-315.
- Berze, J. Eigenartige Gesichtshal uzinationen in einem Fal e von akuter Trinkerpsychose.
Z. ges. Neural. Psychiat., 1923, 84, 487-521.
- Ceroni, L. L'intossicazione mescalinica. (Autoesperienze.) Riv. sper. Freniat.,1932, 56, 42-104.
- . Claude, H., & Ey, H. La mescaline, substance hal ucinogène. C. R. Soc. Biol., Paris, 1934, 115, 838-841.
- Deschamps, A. Ether, cocaine, hachich, peyotl et démence précoce. Paris: Editions Vega, 1932, p. 210.
- Dybowski, M. Conditions for the appearance of hypnagogic visions. Kwari. psychol.,
1939, 11, 68-94.
- Ebbecke, U. Receptorenapparat und entoptische Erscheinungen. Handb. norm. u.
pathol. Physiol. Berlin: Springer, 1929. Vol. XII, Pt. 1, 233.265.
- El is, H. Mescal, a new artificial paradise. Ann. rep. Smithsonian Instit. 1897, 537-548.
- Engerth, G., Hoff, H., & Pdtzl, 0. Zur Patho-Physiologie der hemianopischen Halluzinationen. Z. ges. Neural. Psychiat., 1935. 152, 399-421.
- Epstein, A. L. Somatologische Studien zur Psychiatrie. Z. ges. Neural. Psychiat., 1933, 146, 525-547.
- Ewald, G. Psychosen bei akuten Infektionen, bei Allgemeinleiden und bei Erkrankung innerer Organe. Handb. Geisteskr., Erganzungshand. Berlin: Springer, 1939. Pt. 1, pp. 205-247.
- Fischer. O. Ein weiterer Beitrag zur Klinik und Pathogenese der hysterischen Dysmegalopsie. Mschr. Psychiat. Neural., 1907, 21. 1-19.
- . Forster, E. Selbstversuch mit Meskalin. Z. ges. Neural. P.sychiat., 1930, 127, 1-14.
- Franke, G. Vari erte Serienversuche mit Meskalin. Z. ges. Neural. Psychiat., 1934, 150, 427-488.
- Gurewitsch, M. Über das interparietale Syndrom bei Geisteskrankheiten. Z. ges.
Neural. Psychiat., 1932, 140, 593.603.
- Gurewitsch, M. Weitere Beitrage zur Lehre vom interparietalen Syndrom bei Geisteskrankheiten. Z. ges. Neural. Psychiat., 1933, 146, 126-144.
- Guttmann, A. Medikamentdse Spaltung der Persönlichkeit. Mschr. Psychiat. Neural.
1924, 56, 161-187.
- Guttmann, E. Artificial psychoses produced by mescaline. J. ment. Sci., 1936, 82. 203-221.
- Guttmann, E., & Maclay, W. S. Mescalin and Depersonalization. 1. Neural. Psychopath., 1936, 16, 193-212.
- Haack, K. Experimental-deskriptive Psychologie der Bewegungen, Konfigurationen und Farben unter Verwendung des Flimmerphaenomens. Berlin: Karger, 1927, p. 263.
- Hoff, H., & Pdtzl, O. Über Störungen des Tiefenschens hei zerebraler Metamorphopsie.
Mschr. Psychiat. Neural., 1935, 90, 305-326.
- Hoff, H., & Pötzl, O. Zur diagnostischen Bedeutung der Polyapie bei Tamoren des Occipitalhirnes. Z. ges. Neural. Psychiat., 1935, 152. 483.450.
- Hoppe, I. Der entoptische Inhalt des Auges und das entoptische Sehfeld beim
hallucinatorischen Sehen. Allg. Z. Psychiat., 1887, 48, 438-452.
- Jaensch, E. R., et a!. Grundformen menschlichen Seins. Berlin: Eisner. 1929, pp. xv +
524.
- Jankowska, H. Eidetische Bilder und Halluzinationen. Kwart. psychol., 1939, 11, 189-230.
- Kanner, L., & Schilder, P. Movements in optic images and the optic imagination of movements. J. nerv. ment. Dis., 1930, 72, 489.517.
- Klein, R. Beitrag zur Frage der hemianopischen Halluzinationen. Mschr. Psychiat.
Neural., 1986, 92, 131-149.
- Klein, H. Entoptische Wahrnehmung des retinalen Pigmentepithels im Migräneanfall? Z.
ges. Neural. Psychiat., 1917, 36, 323-334.
- Klüver, H. Mescal visions and eidetic vision. Amer. J. Psychol., 1926, 87, 502-5 15.
- Klüver, H. Mescal. London: Kegan Paul, 1928, p. 111.
- Klüver. H. Fragmentary eidetic imagery. Psychol. Rev., 1930, 37, 441-458.
- Klüver. H. Eidetic phenomena. Psychol. Bull., 1932, 29, 181-203.
- Klüver, H. The eidetic type. Proc. Ass. Res. nerv. & ment. Dis., 1933, 14, 150468.
- Klüver. H. The study of personality and the method of equivalent and non-equivalent stimuli. Character & Pers., 1936, 5, 91-112.
- König, A. Line bisher noch nicht bekannte subjective Gesichtserscheinuflg. Arch.
Ophthal., 1884, 80, 329-330.
- La Bane, W. The peyote cult. New Haven: Yale Univ. Press, 1938, p. 188.
- Ladd-Franklin, C. Visible radiation from excited nerve fiber: the reddish blue arcs and the reddish blue glow of the retina. Science, 1927, 66, 239.241.
- Lindemann, E. The neurophysiological effect of intoxicating drugs. Amer.Psychiat., 1934, 18, 1007-1037.
- Lindemann, E., and Malamud, W. Experimental analysis of the psycho-pathological effects of intoxicating drugs. Amer. J. Psychiat., 1934, 13, 853-879.
- Ludlow, F. The hasheesh eater. New York: Rains, 1903, p. 371.
- Maclay, W. S., & Guttmann, E. Mescaline hallucinations in artists. Arch. Neural.
Psychiat., Chicago, 1941, 45, 130-137.
- Maclay, W. S., Guttinann, E., & Mayer-Gross, W. Spontaneous drawings as an approach
to some problems of psychopathology. Proc. roy. Soc. Med., 1938, 31, 1337-1350.
- Maloney, W. J. M. A. Locomotor ataxia (tabes dorsalis). New York, London: Appleton, 1918, p. 299.
- . Marinesco. G. Recherches sur l'action de la mescaline. Presse méd., 1933, 41. 1433-1437.
- Marinesco, M. G. Visions colorées produites par la mescaline. Presse méd., 1933, 41, 1864-1866.
- Marshall, C. R. Entoptic phenomena associated with the retina. Brit. J. Ophthal., 1935, 19, 177-201.
- Marshall, C. R. An enquiry into the causes of mescal visions. J. Neural. Psychopath., 1937, 17. 289-304.
- Mayer-Gross. W. Psychopathologie und Klinik der Trugwahrnehmungen. Handb.
Geisteskr., ed. by Bumke. Berlin: Springer, 1928. Vol. I, Pt. 1, pp. 427-507.
- Mayer-Gross, W., & Stein, H. Ober einige Abanderungen der Sinnestatigkeit im Meskalinrausch. Z. ges. Neural. Psychiat., 1926, 101, 354-886.
- Menninger-Lerchenthal. E. Das Truggebilde der eigenen Gestalt., Abh. Neur. Psychiat., Psychol. u. ihren Grenzgeb.. 1935, 74, pp. iv + 196.
- Möller, A. Einige Meskalinversuche. Acta psychiat. et. neur., 1935, 10. 405-442.
- Morgenthaler. W. Über Zeichnungen von Gesichtshal uzinationen. Z. ges. Neural.
Psychiat., 1919, 45, 19-29.
- Morael i, G. E. Contribution a la psychopathologie de l'intoxication par la mescaline. J.
de Psychol., 1936, 33, 368-392.
- Mourgue, R. Neurobiologie de l'hallucination. Bruxel es: Lamertin, 1932, p. 416.
- Neuhaus, W. Makropsie und Mikropsie hei Basedowoiden. Z. ges. Neural. Psychiat., 1926, 105, 257-313.
- Pap. Z. v. Einwirkung des Meskalinrausches auf die posthypnotischen Sinnestäuschungen. Z. ges. Neurol. Psychiat., 1986, 155, 655-664.
- Pisk. G. Zur Frage der Pseudohalluzinationen bei der Schizophrenic und ihrer Beziehungen zur eidetischen Anlage. Mschr. Psychiat. Neurol., 1936, 92, 150-156.
- Pdul, O. Tachystoskopisch provozierte optische Hal uzinationen bei einem Falle von Alkoholhalluzinose mit rückgebildeter zerebraler Hetnianopsie. Jahrb. Psychiat. Neural., 1915, 35, 141-146.
- Pötzl, O. Experimentel erregte Traumbilder in ihren Beziehungen zum indirekten
Sehen. Z. ges. Neural. Psychiat., 1917, 37, 278-349.
- Pötzl, O., & Urban, H. Über die isoliert erhaltene temporale Sichel bei zerebraler Hemianopsie. Mschr. Psychiat. Neural., 1936, 92, 67-106.
- Purkinje. J. E. Opera omnia. Prague: Society of Czech Physicians. 1918. Vol. 1, pp. 1-162.
- Rohracher, H. Ueber subjektive Lichterscheinungeus, bei Reizung mit Wechselstromen.
Z. Sinnesphysial., 1935-1936, 66, 164-181.
- Schilder, P. Über monokuläre Polypie bei Hysteric. Dtsch. Z. Nrvenheilk, 1920, 66, 250-260.
- Schilder, P. Über Halluzinationen. Z. ges. Neural. Psychiat., 1920, 53, 169-198.
- Schilder, P. Psychoanalyse und Eidetik. Z. Sex.-Wiss., 1926, 13, 56.
- Schilder, P. Experiments on imagination, after-images and hal ucinations. Amer. J.
Psychiat., 1933, 13, 597-609.
- Schilder, P. The vestibular apparatus in neurosis and psyclsosis. J. nerv. ment. Dis., 1933, 78, 1-23, 137-164.
- Schroder, P. Das Halluzinieren. Z. ges. Neural. Psychiat., 1926, 101, 599-614.
- Serko, A. Im Mescalinrausch. Jahrb. Psychiat. Neural., 1913, 34, 355-366.
- Serko, A. Über einen eigenartigen Fal von Geistesstorung. Z. ges. Neurol. Psychiat., 1919, 44, 21-78.
- Skworzoff, K. Doppelgänger-Halluzinationen bei Kranken mit Funktionsstorungen des Labyrinths. Z. ges. Neural. Psychiat., 1931. 133, 762-766.
- Stein, J. Über die Veränderung der Sinnesleistungen und die Entstehung von Trugwahrnehmungen. Handb. Geisteskr., etl. by Bumke. Berlin: Springer, 1928. Vol. I, Pt. I, pp. 352-426.
- Stockings, G. T. A clinical study of the mescaline psychosis, with special reference to the mechanism of the genesis of schizophrenic and other psychotic states. J. ment. Sci., 1940, 86, 29-47.
- Szuman, S. Analiza formalna i psychologiczna widzen meskalinowych. Kwart. Psychol., 1930. 1, 156-212. Cf. summary in German, pp. 214-220.
- Urban, H. Zur Physiologie der Okzipitalregion des Menschen. Mschz. Psychiat. Neural., 1935, 92, 32-39.
- Urbantschitsch, V. Über subjektive optische Anschauungsbnder. Leipzig, Wien: Deuticke. 1907, pp. vi + 211.
- Urbantschitsch, V. Über subjektive Horerscheinungen und subjektive optische Anschauungsbilder. Leipzig. Wien: Deuticke, 1908, pp. iv + 123.
- Veit, F.. & Vogt, M. Die Verteilung subcutan verabreichter Alkaloide auf verschiedene Regionen des Zentralnervensystems. Naturwiss., 1934. 22. 492-494.
- Vogt, M. Die Verteilung von Arzneistoffen auf verschiedene Regionen des Zentralnervensystems. zugleich ein Beitrag zu ihrer quantitativen Mikrobestimmung im Gewebe. II. Mitteilung: Chinin and Mezkalin. Arch. exp.Path. Pharmak., 1935, 178, 560-576.
- Walton, R. P. Marihuana. Philadelphia: Lippincott, 1938, pp. ix ± 228.
- Weil, A. Die optischen Wahrnehmungsphänomene in der Hypoglykaemie. Mschr.
Psychiat. Neural., 1938, 100, 98-128.
- Wilson, S. A. K. Neurology Baltimore: Wil iams & Wilkins, 1940. Vol. I, pp. xxxvi + 751.
- Wolfe, H. F., & Curran, D. Nature of delirium and al ied states. Arch. Neural. Psychiat., Chicago, 1935, 83, 1175-1215.
- Zádor, J. Meskalinwirkung auf das Phantornglied. Mschr. Psychiat. Neural., 1930, 77.
71-99.
- Zádor, J. Meskalnwirkung bei Storungen des optischen Systems. Z. ges. Neural.
Psychiat., 1930, 127, 30-107.
- Zucker, K. Über die Zunahme spontaner Halluzinationen nach Meskalin. Zentbl. ges.
Neural., Psychiat., 1930. 56. 447-448.
- Zucker, K. Versuche mit Meskalin an Halluzinanten. Z. ges. Neural. Psychiat., 1930, 127, 108-161.
- Zucker, K., & Zádor, J. Zur Analyse der Meskalin-Wirkung am Normalen. ges. Neural.
Psychiat., 1930, 127, 15-29.
Download Our Free Psychedelic Healing Books