The Relation of Expectation and Mood to Psilocybin Reactions
By R.Metzner, G.Litwin & G.M.Weil, 1965
In the rapidly growing literature on the effects of the 'hallucinogenic' or 'consciousness-altering' drugs increasing attention is being paid to the role of non-pharmacological variables. Several authors have pointed to the importance of personality variables in determining drug reactions, and recently these have become the object of systematic study (e.g., Kornetsky and Humphries, 1957; von Felsinger, Lasagna and Beecher, 1955; DiMascio, Rinkel and Leiberman, 1961). Others have emphasized the importance of the physical and social environment (e.g., Hyde, 1960) and the attitude and expectations of the researcher (e.g., Malitz a al., 1960).
The role of these non-drug factors in drug-reaction patterns has recently been reviewed through extracts from the literature by DiMascio and Klerman (1960) and Unger (1963).
In a previous study (Leary et al., 1963) it was found that by deliberately arranging the setting to be warm, supportive and free from distractions, experiences with psilocybin were produced that 70% of the subjects (N = 98) described as "very pleasant" or "ecstatic," and 62% claimed changed their lives for the better. These results are consistent with findings by Ditman a al. (1962) on claims following LSD.
The degree of pleasantness and change was directly correlated with the perceived supportiveness and warmth of the situation. There was also evidence that the pre-drug expectations and mood of the subject were highly correlated with his post-drug reactions. This evidence was not definitive (a) because all information about pre-drug states was obtained after the experience and therefore presumably subject to a 'halo' effect; and (b) because the questionnaire used covered only dimensions such as pleasantness and amount of learning and was non-specific as to content.
The present study was therefore designed to measure the subjects' expectations before the experiment and to correlate these with post-drug responses. Measures of some situational and constitutional variables were also included in the study in order to assess to what extent they affect the pre-drug expectations and the post-drug responses. The hypotheses to be tested were:
- The 'set' of the subject affects the content of the experience: a positive, relaxed 'set' will tend to lead to pleasant experiences and closeness to the other participants; and conversely, an anxious and negative "set" will tend to lead to fearful experiences and distrust or suspicion of the other participants.
- Factors such as age, body-type, previous experience with drugs, and size of the group in which the drug is taken affect the content of the drug-experience.
- Preoccupation with extraneous thoughts or problems will tend to lead to a confused, unpleasant experience.
- Pre-drug mood will affect the content of the experience and the mood during the drug state.
- Specific expectations as to the content of the experience will to some extent determine the nature of the drug-experience.
Not only the expectations of subjects but also the expectations of the researcher may exert a considerable influence on the nature of the drug reactions. The expectations of the researcher may influence the outcome of any experiment (and particularly of a drug experiment) in several ways: through the kind of setting he arranges for the experiment, through the information and attitude he conveys to the subject about his experiment and through his own behavior during the experiment. It is likely that the divergence of results reported by different investigators of the hallucinogenic drugs can in part be explained by experimenter bias.
Some have reported that these drugs are 'psychotomimetic' (e.g., Rinkel
et al., 1952; Malitz
et al., 1960); their experiments have typically taken place in a psychiatric hospital where the subject is surrounded by all the precautions appropriate to 'psychosis.'
Others have used the same drugs in psychotherapy (e.g., Abramson, 1960; Cohen, 1959); here the placebo effect is operating — experimenter and subject want and expect change. A third group of investigators (Wasson, 1961; Savage
et al., 1962) talk of these substances as inducing 'religious' or 'transcendent' experiences. It is clear that the effects of the 'sacred' mushroom taken in the context of a religious ceremony in Mexico will be very different from the effects of the same chemical substance taken in a modern laboratory setting.
Experimenter bias in human experiments is virtually impossible to eliminate (cf. Rosenthal, 1961). One way of controlling it is to vary it for different subjects and measure the effects. This was not attempted in the present study. We adopted the alternative of making our attitudes explicit and constant for all subjects. The setting provided was warm, supportive and non-task-oriented. Pleasant experiences and insight were anticipated. It should be clear that the present study is not an experimental comparison of the effects of psilocybin and a "placebo" under "double blind" conditions, and thus cannot answer the kinds of questions such an experiment could answer. Rather, this is a study of some antecedent-consequent relationships within a single fairly well-planned set of conditions. In this sense it is not an experiment at all, but a study of a certain experience in a particular setting.
EXPERIMENTAL METHOD
The questionnaire was administered to a total of 82 subjects who were given psilocybin. Some of the experimental sessions were part of a rehabilitation program conducted at a state prison. Others were experimental sessions, specifically prepared with this study in mind, in which graduate students or faculty members participated as subjects.
All subjects were unpaid volunteers. Where more than one questionnaire was available on those subjects who were given the drug more than once, the one included in the analysis was selected at random. Occupationally, the sample consisted of 26 prisoners, 25 graduate students, 4 university teachers, and 27 others such as housewives, secretaries, and semi-professional people (research subjects, etc.).
All subjects took the drug in groups: 47 subjects in all male groups (all the prisoners), and 35 in mixed groups. In the present study 59% were first experiences (with psilocybin, mescaline, or LSD) , 15% were second experiences, and only 5% had five or more previous experiences. The distribution of age in years was approximately normal, with a mean of 26.9 and a standard deviation of 7.1.
SELECTION AND PREPARATION
Subjects who volunteered for the study were given medical screening by the University Health Services or the prison psychiatrist. Psychological screening was done by a group of psychologists. All were interviewed individually before the experiment, the purpose of the particular project in which they were participating was discussed, and subjects themselves participated in determining the composition of the group. Whenever possible it was arranged so that every participant had at least one close friend present, was not with people who disliked each other, or with total strangers.
It was thought that this would maximize the chances of having a warm, supportive setting. Before the experiment, the whole group met at least once (in the case of the prisoners up to three or four times) for two to three hours for open discussion and for the purpose of acquainting the group members with one another. Subjects were told what drug they were getting and what was known about it; they were encouraged to do background reading. They were told to make 5-6 hours of time available, free from distractions or interruptions.
No manipulation was performed by the experimenters without knowledge of the subject. All groups contained at least one subject who had previous experience with psilocybin and who was able to guide initial subjects through their experiences, if this became necessary. The pre-drug section of the questionnaire was filled out by the subjects before ingestion; the main part after the session had ended.
SETTING
All non-prison sessions were conducted in comfortable home surroundings in an attempt to create a relaxed and comfortable atmosphere. Living rooms of a moderate-to-large size were used. Easy chairs, rugs and cushions formed the basic furnishings. Recorded music, books and paintings or prints were made available. Food and drink were also offered.
Prison sessions were conducted in a large separate room in the prison hospital. The room was furnished with beds, mattresses, tables and chairs. Recorded music, prints and books were also made available.
DOSAGE
Subjects were told the standard and maximum dosages and were then permitted to regulate their own dosage. The mean dosage for the whole sample was 0.39 mg per kg, with a standard deviation of 0.35. For an adult of average size and weight this represents an average dosage of between 25 and 30 mg.
THE QUESTIONNAIREPART I: Pre-drug section / Background variables
Subjects were asked to state how many people were present, how many actually took the drug, what their occupation, sex, age, height and weight were, what previous experiences they had had with similar drugs, and what dosage they were taking in this session. For the subjective 'set', subjects were asked to state:
- How apprehensive are you about taking the drug today?
(Very apprehensive / slightly apprehensive / not anxious at all)
- To what extent are you preoccupied with thoughts or problems not connected with this session? (0 not at all; to 4 very much)
- How good do you feel about taking the drug today? (Not good / neutral / good / great)
- A set of 12 phrases describing specific reactions. The subject is asked to check those he expects to experience.
- Pre-drug Mood Adjective Check-List. This is a 48-item check-list derived from the factor-analytic studies on mood of Nowlis et al. (1957). For each of the factors extracted, the adjectives with the six highest loadings were used, and each mood score is the sum of these six items (items with negative loadings were subtracted). Each item could be answered from 0 = "does, not apply" to 3 = "applies very strongly to my present mood". The composition of the mood scales is shown in Appendix A.
PART II Post-drug section
At the end of the session the subject filled out the same mood adjective check-list again, to describe how he felt at the height of the drug experience. Then followed a list of 108 specific content items (see Appendix B) , each of which can be answered by:
0 = did not occur
1 = occurred once or only a little
2 = occurred quite a lot,
3 = among the most important aspects of my experience.
The items were derived (a) from reports written by other subjects and in the literature, (b) from personal experiences, (c) from theoretical suppositions and (d) from observations of subjects.
They were intended to cover the widest possible range of experiences, and were grouped according to a set of 12
a priori categories (the composition of the categories is shown in
Appendix C):
- somatic symptoms (16 items)
- perceptual transformations (14 items)
- perceptual hallucinations (7 items)
- hallucinations involving the whole person (18 items),
- unusual cognitive phenomena (15 items),
- religious or mystical phenomena (8 items)
- interpersonal-positive (7 items)
- interpersonal-negative (7 items)
- drug concerns (3 items)
- primary processes (9 items plus all hallucinations and perceptual transformations)
- paranoia and ideas of reference (8 items)
- empathy or insight (7 items).
METHOD OF ANALYSIS
Means, standard deviations and intercorrelations of all variables were obtained. The basic results will be presented and discussed in five separate sections. First, most and least frequent categories are presented to give a general picture of the range of experiences in the group sessions. Second, the correlations of background variables to specific experience items are presented. Third, the correlations with subjective "set," and fourth, the correlations with specific expectations will be described. Finally, the mood data are described in terms of the relation of pre-session mood to mood in the session, and to specific response items.
RESULTS
PART I: Most And Least Frequent Responses
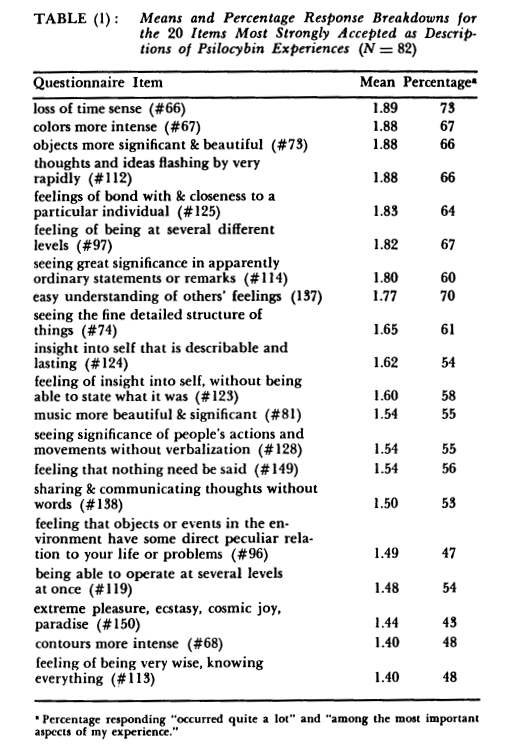
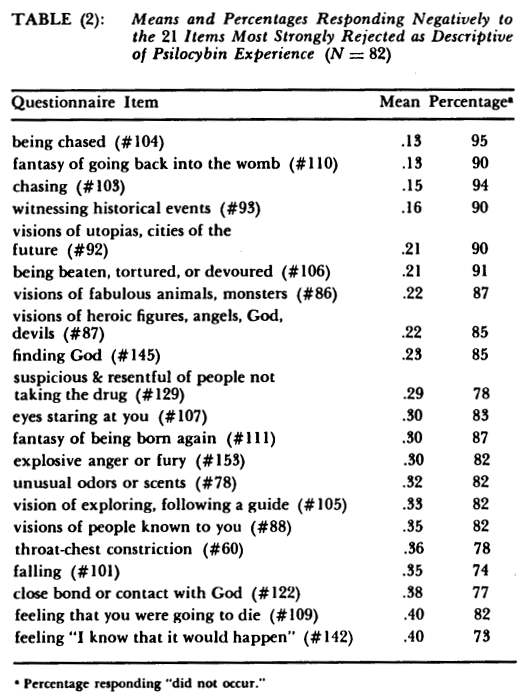
The twenty items most frequently accepted and rejected as descriptions of psilocybin experiences are shown in Tables (1) and (2) respectively. In terms of the a priori grouping of items it may be noted:
- That somatic items are neither accepted nor rejected very often, but are reported as occurring mildly in most subjects;
- That five of the most frequently checked items indicate perceptual transformations; only one perceptual transformation item (#78) is in the least frequent category;
- None of the most frequent items are "hallucinations" whereas 14 of the least frequent items are;
- Four of the most frequent items are in the category of "increased interpersonal sensitivity" (#125, 137, 128, 138) , whereas no negative interpersonal items are reported;
- Two of the items in the most frequent group (#66 and 96) are indications of primary process functioning; others (#112, 97, 119, 123) are representative of unusual cognitive phenomena.
DISCUSSION
The finding that somatic symptoms, while they do occur, are not a primary component accompaniment of reported psilocybin experiences suggests that the peripheral autonomic effects of psilocybin are relatively minor compared to the central effects. Perceptual transformations and interpersonal sensitivity were more prominent aspects of the experience. The relative paucity of reported hallucinations was surprising, and suggests that the term "hallucinogenic" for these substances is somewhat misleading. The positive interpersonal effects are probably attributable largely to the group setting and preparation the subjects underwent before the sessions.
The common theme linking the most frequent items seems to be increased awareness or perception of deeper meaning (#73, 74, 81, 96, 97, 113, 114, 119, 124, 137). Four other items (#123, 128, 138, 149) , which refer specifically to an increase in intuitive nonverbal thinking, may also be included in this category. People, events, objects, one's self seem to be more clearly understodd, although this understanding is difficult to convey verbally to others.
PART II: AGE, BODY-TYPE, PREVIOUS EXPERIENCE, GROUP SIZE, AND DOSAGE
(A) Age Differences: Older subjects tended slightly to have had more previous drug experiences (r = .20), to be more endomorphic (r = .32), to be more preoccupied with other things before the session (r = .29) and to expect depression less (r = —.20).
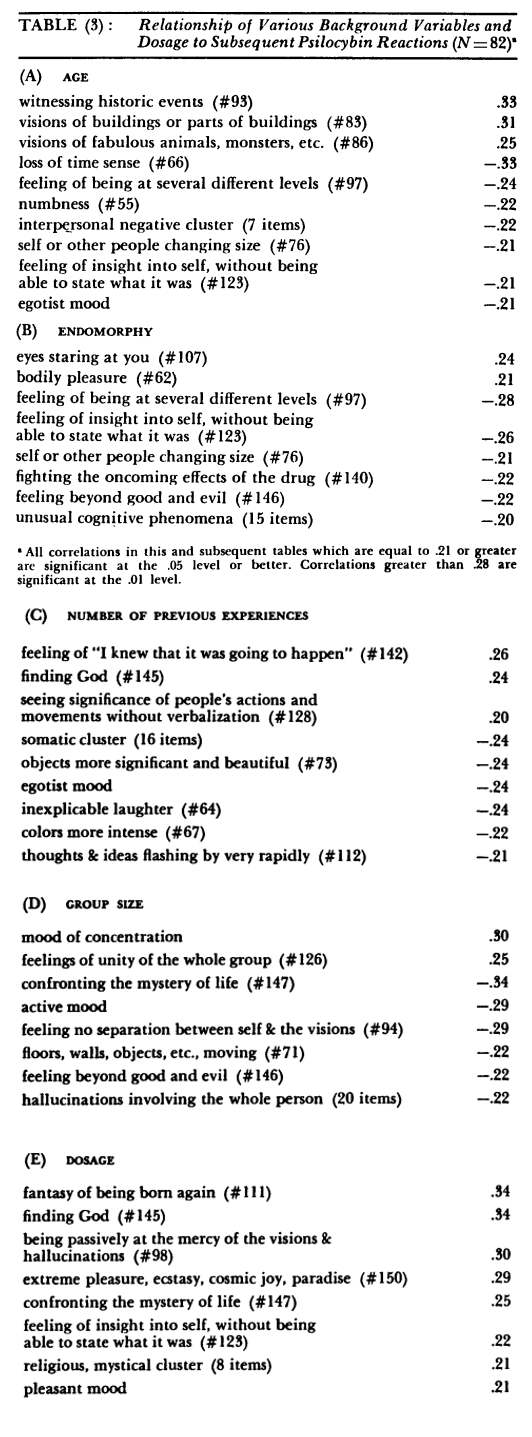
The correlations with post-drug reactions are shown in Table (3). The only mood difference is that older subjects tended to report less "egotism". There are significantly more historical and mythical visions in older Ss and less of the typical time confusion.
Older subjects tend to report fewer negative interpersonal experiences (r = —.22); this cluster includes items such as "feeling left out and isolated" and "fear of being thought silly or stupid or crazy."
(B) Body-Type Differences: The crude index of endomorphy used here, weight divided by height, has a mean of 2.26 pounds per inch for the whole sample, with a standard deviation of 0.29; it is approximately normally distributed. Endomorphy in this sample is related positively to age (r = .32) and to sex (r = .71), men being more endomorphic. The prisoners also are more endomorphic than the non-prisoners (r = .23) . Endomorphs tend not to expect ecstasy, love or depression, are less likely to be "affectionate" in their pre-drug mood (r = —.30).
From Table (3) it can be seen that endomorphs report more "bodily pleasure"; this item is not correlated with age or sex. There is also an almost significant negative correlation between endomorphy and the cluster of unusual cognitive items as a whole.
(C) The Effect Of Previous Experience: Since this variable was so markedly skewed in its distribution, all significant relationships were also tested by chi-square. A three-way breakdown was made into three groups: (a) 48 Ss with no prior experience with drugs, (b) 19 Ss with one or two prior experiences, and (c) 15 Ss with three or more previous experiences.
Only relationships which were significant by both methods of analysis will be discussed.
The more experienced subjects tend to expect "ecstasy" and "love" more often than the inexperienced (r = .25 and .27, respectively). When the distribution is broken down into thirds it can be seen that this correlation is primarily due to the responses of the group with three or more previous experiences.
As Table (3) shows, number of previous experiences is significantly negatively related to egotism on the mood scale, and also negatively to the cluster of somatic symptoms. Perceptual transformations such as "colors more intense" or "objects more significant and beautiful" are reported less frequently by the more experienced subjects; analysis using chi-square shows this to be a trend occurring primarily in the upper third of the distribution. The other relationships shown in Table (3) are nonsignificant when analyzed by chi-square.
(D) The Effects Of Group Size:
The size of the groups ranged from two to thirteen with a mean of six. Almost 50% of the subjects participated in groups of either five or six members. In view of this restricted range these data are not a very sensitive measure of the effects of group size, and the data should be regarded as suggestive only.
Group size is significantly related to number of stated expectancies (r = .24); i.e. the larger the group, the more things subjects expect to happen. Specifically, to participate in larger groups is to expect more visual changes (r = .38), more ecstasy (r = .21) and more depression (r = .21) On the pre-drug mood scales, subjects in larger groups are higher in concentration, and lower in pleasantness, activation and egotism.
Table (3) shows that large group experiences involve more concentration and less activation. Feelings of group unity tend to be greater in the larger groups, but the more personal subjective phenomena appear to be less frequent.
(E) The Effects Of Dosage:
There was no correlation between dosage taken and previous drug-experience. Taking a high dose is negatively related with expecting "loss of reality" (r = —.20) . Taking a higher dosage is correlated positively with pre-drug moods of social affection (r = .22) , depression (r = .20) and anxiety (r = .30).
Table (3) shows the correlations with post-drug effects. The higher dosage tends to produce experiences that are more pleasant and more mystical or religious. Experiences of being reborn or finding God (which are rare in general) are more likely after higher dosages.
DISCUSSION
The results show that a number of background and constitutional variables have significant effects on the contents of the psilocybin reactions. The major conclusions may be summarized as follows:
- Older subjects report more historical and mythical visions and less time confusion than younger subjects.
- Endomorphic subjects report "bodily pleasure" more often and unusual cognitive phenomena less often than ectomorphs. This finding is consistent with the report of DiMascio et al. (1961) that "athletic," mesomorphic subjects have more physiological effects and euphoria, and less intellectual impairment than "aesthetic" subjects.
- Subjects who have had previous experience with hallucinogenic drugs differ from inexperienced subjects (a) in having fewer somatic symptoms, (b) in being less 'egotistic' in mood, and (c) in reporting fewer perceptual transformations.
- Subjects in larger groups report feelings of group unity more often and subjective hallucinatory phenomena less often than subjects in smaller groups. It is possible to interpret this as indicating that in the larger groups more energy is taken up with interpersonal interaction and therefore fewer of the purely subjective phenomena are reported.
- The effect of having taken higher dosages was to increase the frequency of religious, ecstatic and mystical experiences.
These background variables also affect the pre-drug set, expectations and moods of the subjects significantly. For example, (a) the more experienced subjects expect ecstasy and love more .34 often, and (b) subjects who take higher dosages expect "loss of reality" less often.
PART III: THE EFFECTS OF SUBJECTIVE SET
(1) Pre-drug Anxiety:
Answers to the question, "How apprehensive are you about taking the drug today?" were scored from 1 ("not anxious at all") to 3 ("very apprehensive").
This score, the "anxiety" index, correlated .22 with the stated expectation of "depression" and .21 with the "anxiety" score derived from the pre-session mood check-list.
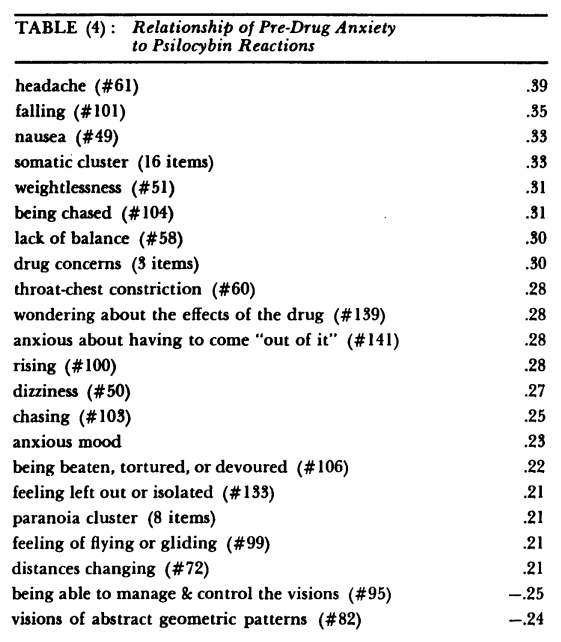
As Table (4) shows there is a positive correlation of pre-drug anxiety with "anxious" mood during the session (r = .23). There is a highly significant correlation with the cluster of somatic symptoms (r = .33), of which the two most important items are headache and nausea.
Experiences of "falling" which are reported in only 26% of the total sample, are highly correlated with pre-drug anxiety. Concerns about the drug (#139, 141) figure largely in these experiences, as do distrustful ideas about the other subjects (#107, 133), and self-punitive reactions such as "being beaten" and "being chased".
The negative correlation with the item "being able to manage and control the visions" (r = -.25) suggests that anxiety about loss of control is a source of this kind of experience.
(2) Preoccupation: The extent of preoccupation with thoughts and problems not related to the session was scored from 0 ("none") to 4 ("a great deal"). This index is positively correlated with age (r = .29), i.e. older subjects tend to be more preoccupied; with the expectation of "loss of inhibition" (r = .24) and with "depression" (r = .25) on the pre-drug mood check-list.
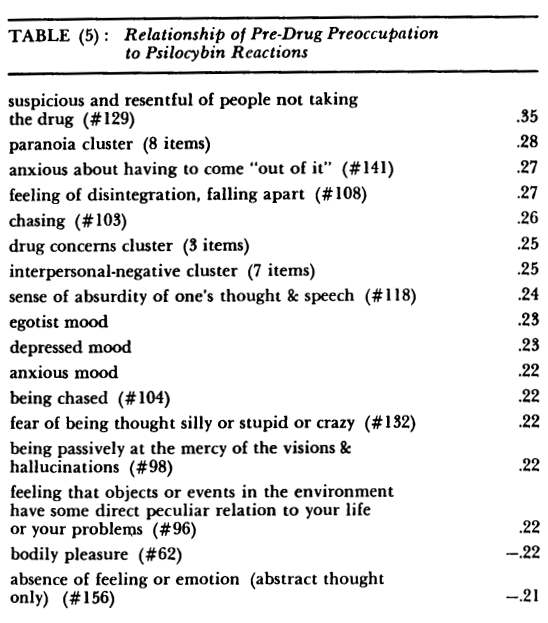
From Table (5) it can be seen that the extent of preoccupation correlates with experiences of distrust, confusion, drug concerns, anxiety, and depression. It differs from the syndrome following pre-drug anxiety primarily in the absence of somatic complaints.
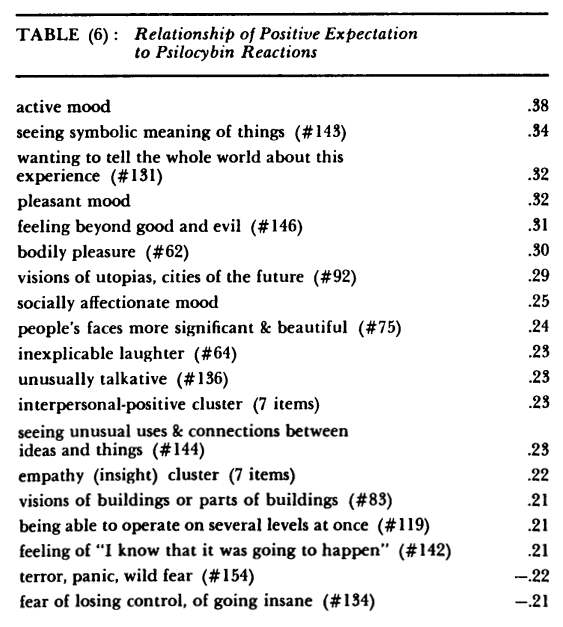
(3) Positive Expectation:
Answers to the question, "How good do you feel about taking the drug today?" were scored on a four-point scale as follows: 0 = not good, 1 = neutral, 2 = good, 3 = great. This score correlated negatively with the mood scales "concentration" (r = -.24), "depression" (r = —.40) and "anxiety" (r = —.24); it correlated positively with moods of "pleasantness" (r = .49), "activation" (r = .30) and "affection" (r = .30). Positive expectation is not correlated with the other "set" items, anxiety or preoccupation; nor are these two correlated with each other.
Table (6) shows that activation, pleasantness and affection are the main dimensions of the post-drug mood correlated with positive expectation. Empathy and positive interpersonal experiences are the main focus of these items. Feelings of expansiveness ("wanting to tell the whole truth," "unusually talkative"), "feeling beyond good and evil," bodily pleasure, laughter — and others, characterize a powerful euphoric experience. The déjà-vue experience is also related both to positive expectation and to preoccupation.
DISCUSSION OF SUBJECTIVE SET
Our findings indicate that positive expectations produce pleasant and educational experiences in the drug sessions. The evidence also indicates that negative and anxious experiences are produced by psilocybin if the subject is either anxious about the drug, or preoccupied with other things. Thus hypotheses (1) and (3) are confirmed. Anxiety about the drug tends to produce somatic manifestations. This suggests that the bodily symptoms, beyond those which almost everyone experiences initially, may be, in fact, defensive maneuvers. Blewett and Chwelos (1959) report the observation that the "flight into symptoms" is one of the first lines of defense taken by subjects taking LSD-25 who are anxious about the oncoming effects. Difficulty in controlling the visions is the characteristic trigger of anxiety experiences in subjects who are concerned about maintaining ego-control over their experiences.
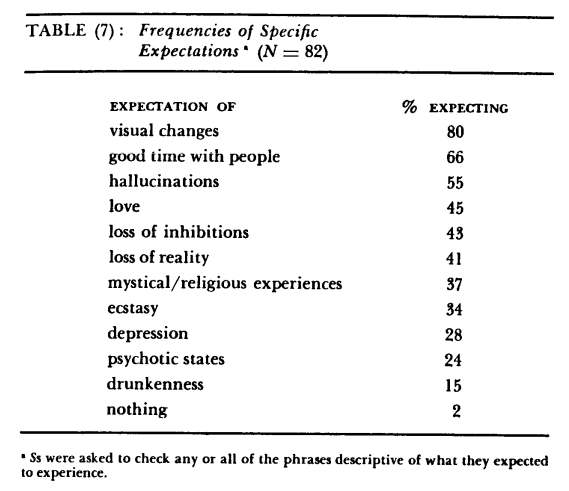
PART IV. THE EFFECTS OF SPECIFIC EXPECTATIONS
The frequency with which each of the 12 categories of expectation was checked is shown in Table (7). This set of expectancies, which is strongly biased towards the positive side, reflects the preparation and setting provided for the subjects. The category "nothing" is not included in further data analyses since there is no meaningful split of the sample on this dimension. "Drunkenness," "psychotic states" and "visual changes" also have strongly skewed distributions in which less than 25% of the subjects fall in one category. However, the correlation coefficients still contain some worthwhile information.
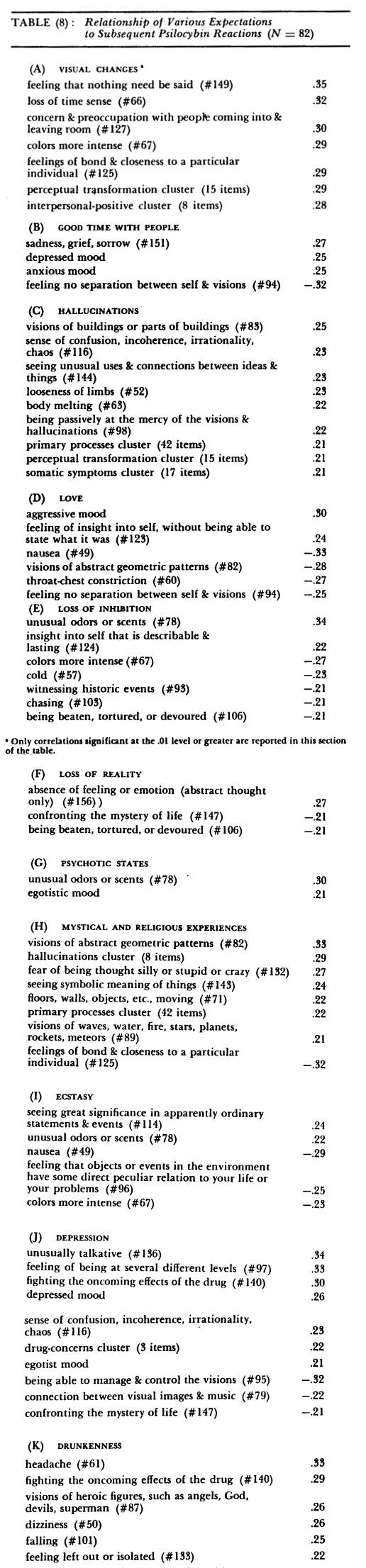
"Visual changes" are expected by 80% of the subjects; hence this item is related to a large number of specific items, especially the ones which occur more frequently. Table (8A) shows only the correlations of .28 and higher (significant at the 1% level): perceptual transformations and interpersonally-oriented items are most strongly correlated with this category. The expectation of "good time with people" tends to produce primarily negative experiences (Table 8B). The expectation of "hallucinations" is correlated with the perceptual transformations cluster and the primary process cluster, which includes hallucinations.
The expectation of "love" is most strongly related to aggressiveness, insight and déjà-vue experiences; expecting love is significantly negatively related to various somatic symptoms, such as nausea, throat-chest constriction and body-melting. In part this may be accounted for by the relationships of these two variables to previous experience.
Subjects with more previous experience tend to expect love more and also to experience fewer somatic symptoms. But there is also an independent correlation, as shown by the partial correlation of —.30 between expecting love and nausea, with previous experience held constant. Expectation of "ecstasy," which is correlated .43 with expecting "love," is also highly negatively related to nausea.
Expecting "loss of inhibition" is primarily related to "unusual odors and scents," which is one of the rare items. Expectations of "loss of reality" and "psychotic states" tend to be checked by the same subjects (r = .50) but seem to have minimal effect: "absence of feeling or emotion" and "unusual odors and scents" are the only very significant items. There is a tendency for these subjects not to experience the mystical aspects.
Subjects who expect mystical or religious experiences tend to report a large variety of perceptual and visionary effects but not necessarily of religious content; they tend not to have the interpersonal empathy experiences.
The expectation of "depression," which is correlated with pre-session anxiety (r = .22) is predictive of confused, depressed experiences marked by attempts to maintain ego-control over the drug effects.
The expectation of "drunkenness" seems to lead primarily to a set of somatic complaints, typical "drunk" effects (headache, dizziness).
DISCUSSION OF SPECIFIC EXPECTATIONS
Some of the results from this analysis are paradoxical: subjects who expect a "good time with people" tend to have negative experiences. Expectations of mystical experiences, of ecstasy and love, are not followed by corresponding experiences. Subjects who expect psychosis or loss of reality are not more likely to report such events.
On the other hand, expectations of visual changes, hallucination, depression and drunkenness tend on the whole to lead to corresponding experiences. Bodily symptoms are more likely to be experienced by those who expect "drunkenness," and less likely by those who expect "ecstasy" or "love." Thus hypothesis (5) is only partially confirmed.
The correlation between expecting "loss of inhibition" and the reported experience of "unusual odors and scents" may be related to Couch and Keniston's (1960) finding that the personality dimension — impulsivity versus control is strongly correlated with an anal syndrome.
PART V: MOOD AND MOOD CHANGES
Scores on the eight mood scales (see Appendix A) were analyzed (a) for mean pre-post changes in the whole sample, (b) for correlation of pre-session mood to mood during the session, and (c) for the relationship between base-rate mood expectancy, pre-session mood, and mood during the session.
Ss indicated their mood during the session by filling out the adjective check-list at the end of the session. The instructions were to describe their mood "at the height of the drug experience."
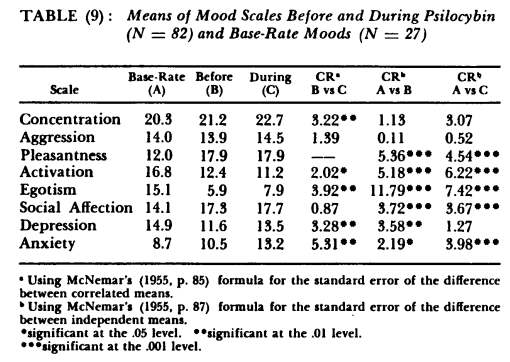
Table (9) shows the means and standard deviations of the mood scales before and during the session. There are significant mean increases in the "concentration," "depression," "anxiety," and "egotism" scales; and decreased mean "activation." In other words it appears at first that there is a significant increase in specifically depressive, anxious and egotistic adjectives which are lowest at the start. The only scale which declines is "activation," i.e., subjects become less energetic and vigorous during the session.
In order to understand more clearly the nature of these mood changes it is necessary to ask the question: how does the mood at the beginning of the session compare with mood during an average day? In order to obtain such base-rates a sample of 27 Ss (15 males, 12 females) similar to the experimental sample in age and socioeconomic status was given the adjective check-list and asked to describe their mood "at this moment." The check-list was collected in the course of a variety of daily activities and the means (shown in the first column of Table 9) may be regarded as base-rate expectancies for these moods independent of experimental set or atmosphere.
From these comparisons it can be seen that the "egotism" and "depression" scales, which increase during the session, are significantly below normal at the start of the session, and the increase does not ever approach the base-rate level.
Conversely, "pleasantness" and "social affection" are, significantly, highly above normal before the session, and do not increase any further during the session.
Of the four remaining scales, "concentration" and "aggression" before the session are not different from normal; "activation" is below normal and "anxiety" is slightly above normal.
In other words, the effect of the present preparation and setting was to increase pleasant and affectionate moods, to decrease depression and egotism, to lower the energy level and to raise the anxiety level. Then, at the height of the drug reaction, pleasantness and affection stay high, depression and egotism increase but stay below base-rate levels, concentration increases, energy decreases still further and anxiety increases.
Another way of viewing these data is to compare the mood at the height of the session with the normal everyday mood of the base-rate sample. The drug subjects report more concentration, more pleasantness and affection and also more anxiety; they feel less egotistic and less active.
VARIABILITY
An index of total variability of mood on the post-drug checklist was derived by simply summing the number of adjectives checked. This measure is related significantly to pre-session moods of "aggression" (r = .40), "social affection" (r = .33), and "pleasantness" (r = .24).
CORRELATIONS WITH SUBSEQUENT RESPONSES
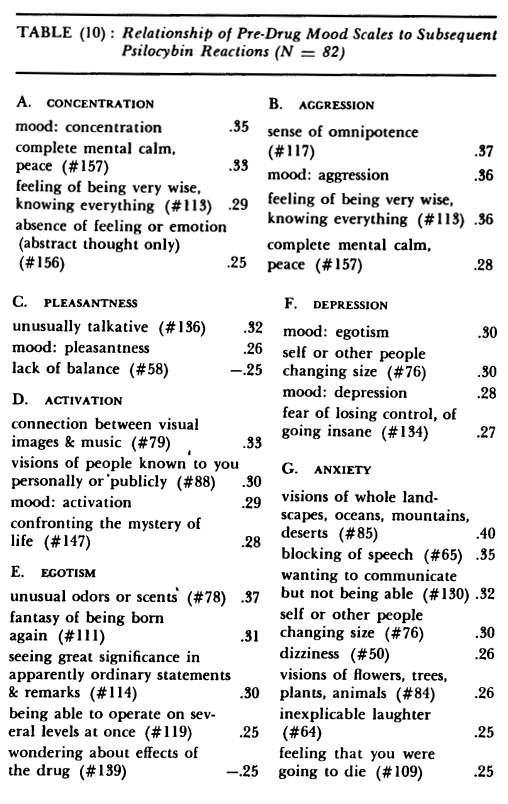
Tables (10) and (11) show the correlation of the pre-drug mood scales to subsequent responses. Only correlations of .25 or higher are shown. In each case, with one exception, the pre-drug mood correlates highly and significantly with the corresponding scale on the session mood-list. The exception is egotism, which only
correlates .14 with post-drug egotism. But in general, the mood of the subject during the session is predominantly determined by his mood before the session.
Initial "concentration" (Table 10) leads to calm, non-emotional experiences. Initial "aggression" leads to feelings of power and omniscience. A "pleasant" mood before the session leads to "talkativeness"; in addition, the following items are correlated (at the .05 level) with pre-drug "pleasantness": pleasure (# 150; r =.24), visions (#92, 105; r = .23), mystical experiences (#145, 147; r = .22 and .21 respectively). "Pleasantness" on the pre-drug mood scale and positive expectation are highly intercorrelated (r = .49).
Pre-drug "anxiety" and "depression" are intercorrelated (r=.52). "Anxiety" leads to blocking, disintegration and perceptual distortions of size (Table 10). Other items correlated (at the .05 level) with "anxiety" are: drug concerns (r = .24), anxious mood during the session (r = .23), objects distorted (#70, r = .22), feeling of disintegration, falling apart (#108, r = .22), sense of omnipotence (#117, r =.21), "depressed" mood (r = .21).
Pre-drug "depression" leads to "egotism" and fear of losing control. The initial expectation of loss of inhibition is also related to pre-drug "depression" (r = .28). Other items correlated (at the .05 level) with "depression" are: visions of waves, water, fire, stars, planets, rockets, meteors (#90, r = .24), anxiety about having to come "out of it" (#141, r = .23), "anxious" mood (r = .22), unusual odors or scents (#78, r = .22), large swings of mood, happiness and sadness (#155, r = .21).
DISCUSSION OF MOOD
The finding for the mood scales in general parallels those obtained from the positive and negative set variables and tends to confirm our hypotheses. The best predictor of mood during the session is mood before the session. The base-rate data are interesting in this respect since they are significantly different from the pre-session moods across most of the scales. These data support our assumption as to the overall effect of the positive set induced in the preparation of our subjects.
For example, "egotism" in the pre-drug assessment is significantly lower than the base-rate, and its slight increase during the session is still significantly below the base-rate. The "egotism" scale is made up of such items as "self-centered," "egotistic," and "boastful." We tentatively suggest that the slight increase in these items during the session forms part of a general syndrome of self-devaluation centered around the inability to maintain control over the experience. The increase in "anxiety" during the session and the relatively small degree of anxiety in the base-rate would seem to support this interpretation.
There seem to be several kinds of mood changes represented in these data. "Concentration" and "anxiety" start at low base-rate, increase significantly in the pre-drug assessment (presumably as a result of the preparation and setting), and increase still further during the drug experience. Conversely, activation is decreased in the pre-drug assessment and decreased still further during the drug experience. On the other hand "pleasantness" and "social affection" are greatly increased in the pre-drug assessment, but increase no further during the drug experience, and may be thought of as specific effects of the preparation and setting. "Egotism" and "depression" are greatly decreased in the pre-drug condition, but increase somewhat during the drug experience.
A negative mood cluster (depressed, anxious) prior to the session tends to lead to negative experiences marked by fear of losing control, size-distortion, feelings of disintegration, inability to communicate and depression. A positive mood cluster leads to a predominately pleasant experience including a number of religious and positive interpersonal aspects. It also leads to a more varied experience (in terms of number of mood adjectives checked). The relation of pleasantness to variability of experience may be seen in light of theories (e.g., Easterbrook, 1959) which propose that one of the effects of emotional tension is to reduce the number of cues utilized in a given situation. Thus anxiety limits the range of awareness and a pleasant, confident mood increases it. The preparation for these experiences in this study included attempts to emphasize and create pleasantness and confidence, and the data demonstrate that these attempts were quite successful.
GENERAL DISCUSSION
Three groups of data have been presented in this paper:
- The most and least frequent categories of response in psilocybin experiences.
- The effects of various background variables and dosage on responses to psilocybin.
- The effects of expectations and mood on responses to psilocybin, which was the main focus of the study.
The results of the comparison between most and least frequent categories indicate that the principal element in these experiences is the increased awareness or perception of deeper meaning. These findings cannot be solely attributed to the desire of the subjects to confirm the expectations of the experimenters. Other investigators (e.g., Linton and Langs, 1962) also report this effect though not as the most frequent. Furthermore we found that certain responses (e.g., hallucination) which we did expect to occur frequently in fact did not. The greater meaning perceived by the subject was often explicitly stated to be non-verbalizable.
Although no one psychological theory is adequate in accounting for such phenomena, they are consistent with views (such as those of Freud, Piaget, the transactionalists and others) which hold that perceptual and cognitive structures are acquired response patterns, with which the organism filters and organizes the enormous and varied input from his environment. Assuming for the sake of argument that it is possible temporarily to disrupt these response-structures, so that the subject "sees" without them, the experience would clearly have the two features found here:
- It would give the feeling of "insight," as perceptual barriers are suddenly broken.
- It would be non-verbalizable precisely because the categories and structures are chiefly verbal response-patterns.
Several specific relationships of background variables to psilocybin responses were reported. Thus older subjects report more historical and mythical visions than younger subjects, and endomorphs report bodily pleasure more often than ectomorphs. These findings should be regarded as suggestive and require further confirmation. The interpretation of these differences would probably involve differences in personality and expectations between these groups.
Subjects with previous experience with hallucinogenic drugs report fewer somatic symptoms and fewer perceptual changes than inexperienced subjects. It may be that with increasing familiarity with the psychedelic experience a subject concentrates more on the interpersonal and intrapersonal changes and the somatic and perceptual manifestation becomes less important.
Three main groups of set variables were analyzed:
- Direct questions or ratings of anxiety, preoccupation and positive anticipation.
- Statements of the kind of experience the subject expected to have.
- Affective states inferred from mood adjectives. Each of these measures was obtained immediately prior to the drug session and correlated with post-drug responses.
The overall results may be summarized as follows:
- Positive expectations lead to positive experiences; anxiety or preoccupation lead to unpleasant experiences; anxiety specifically increases the number of somatic symptoms experienced.
- Statements of specific expectations on the whole are not good predictors of subsequent experience.
- Mood before the session is the best predictor of mood during the session: unpleasant (depressed, anxious) moods are intensified on the whole, pleasant moods lead to pleasant and varied experiences.
- Mood before the session is generally significantly different from base-expectancy and confirms the efficacy of the set-inducing procedure.
It is not clear from the present data why the statements of specific expectations should not be good predictors. It may be that the expectation statements, which were mostly simple, one-word phrases, are concealing more complex sets of cognitive expectancies; thus, perhaps more subtle measures of expectancy would lead to successful prediction.
On the basis of these results a working hypothesis on the nature of set effects could be formulated as follows: the chemical psilocybin initiates a chain of biochemical and physiological events in the central nervous system, the end result of which is the suspension or deactivation of perceptual and cognitive structures involved in categorizing the perceived environment.
The two main sources of stimuli to conscious awareness, the internal state and the external environment, are therefore capable of exerting a much more direct effect since they are not subject to the usual categorizations. In other words, there is greatly increased openness and suggestibility to both 'set' (internal cues) and 'setting' (external cues).
A person may regard the possibility of losing his usual perceptual categories with anxiety, depending on the degree to which these categories are defensive. On the other hand, a person who is relatively free from anxiety will be able to accept a wider range of internal and external stimuli.
This formulation may now be applied to some of the results presented above. The perception of new meaning, non-verbal insights, which are most frequently reported can be seen as a consequence of the temporary suspension of perceptual and cognitive screening structures. The subject "sees" connections hitherto unnoticed. The reduction of defensive barriers, in a situation of trust and confidence, will tend to eliminate the sense of interpersonal distance: this accounts for the correlation of pleasant expectations with experiences of empathy and interpersonal closeness. The increased variability of mood and the specific increase in unpleasant affect can be seen as a consequence of the greater availability of internal cues.
The preparation given to our subjects explicitly included the concept of increased awareness and insight, so that the process of volunteering probably screened out most subjects who are potentially anxious about such an experience.
The majority of studies in this field have tended to use paid subjects, and not to make any preliminary statements about the kinds of experience one might expect. Linton and Langs (1962), for example, gave LSD to subjects who volunteered "for a psychological study in which they might earn money." No further explanations were given. The most "typical" effects reported by them are feelings of losing control over thoughts and annoyance at this "impaired functioning." These are the effects reported by our subjects with negative, anxious anticipation or set.
How can one explain these effects of pre-drug anxiety? As the drug-induced perceptual changes begin to take place, the subject will attempt to deal with them in the usual way, depending on his defensive strategies. He may focus his attention on one limited aspect, e.g., bodily function; he may attribute the effects to outside causes, e.g., he may become suspicious about other participants; or he may resort to self-accusation for failure to control his thoughts and become depressed. All of the responses are correlated with pre-drug anxiety (Table 4).
Two implications for research in this area emerge clearly: first, the expectations of the subjects should be carefully measured before drug administration; and second, the expectations of the experimenters should be stated explicitly in research reports, if results are to be at all comparable and replicable.
Finally we may examine the correlates of mystical or religious experience in the light of this theory. These experiences (e.g., "close contact with God") are reported by about 20% of the subjects (Table 2). Experiences of "unity" or "communality" with other people, with the world as a whole, or with God, may be seen as the end-point on a continuum of perceptions without the intervening controlling or modifying structures. As the discriminating and differentiating processes are suspended, more and more phenomena are "unified." The cluster of religious items is correlated positively with dosage — the higher the dosage, the more likely this effect becomes.
SUMMARY
The results of a questionnaire study of the effects of psilocybin on small groups of volunteers, (N = 82) are reported. The experimental setting was warm and supportive, and the subjects were prepared to expect insight and expanded awareness. The most frequently reported experience within this setting was a perception of "new meaning"; significant differences in the content of the experience as a function of age, body-type, previous experience, group size and dosage were found.
Pre-drug anxiety and positive expectation led to negative and positive experiences respectively. Stated expectancies did not have a marked effect on the experience. Pre-drug mood had very pronounced effects on mood during the session: depression or anxiety, if present before, was increased; pleasant moods led to pleasant and varied experiences.
A working hypothesis was proposed according to which the effect of psilocybin is to suspend or deactivate temporarily the cognitive-perceptual screening structures. This hypothesis was applied to account for the effects of expectation and mood on drug experience.
NOTES
The research reported in this paper was supported in part by a grant from the Laboratory of Social Relations, Harvard University. Grateful acknowledgement is made to Richard Alpert and Timothy Leary for their advice and encouragement.
FURTHER READING
- Abramson, H. A., ed. The Use of LSD in Psychotherapy. Josiah Macy, Jr. Foundation, New York, 1960.
- Blewett, D. B. & Chwelos, N. Handbook for the Therapeutic Use of LSD. Mimeographed, 1959. (Saskatchewan, Canada) .
- Cohen, S. The therapeutic potential of LSI)-25. In A Pharmacologic Approach to the Study of the Mind. Ed. Featherstone, R. M. Springfield: C. C. Thomas, 1959, pp. 251-257.
- 34 Expectation, Mood and Psilocybin Reactions
- Couch, A. S. & Keniston, K., Yeasayers and Naysayers: Agreeing Response Set as a Personality Variable. 7. Ab. Soc. Psychol., 1960, 60, pp. 151-174.
- DiMascio, A. & Klerman, G. L. Experimental human psychopharmacology: the role of non-drug factors. In Dynamics of Psychiatric Drug Therapy, ed. Sarwer-Foner, G. J. Springfield, 111.: C. C. Thomas, 1960, pp. 56-85.
- DiMascio, A., Rinkel, M. & Leiberman, J. Personality and Psychotomimetic Drugs. Psychopharmacology Research Laboratory, Massachusetts Mental Health Center, Boston, Research Report, 1961.
- Ditman, K. S., Hayman, M. & Whittlesey, J. R. B. Nature and Frequency of Claims Following LSD. 7. Nerv. Ment. Dis., 1962, 139, pp. 346-352.
- Easterbrook, J. A. The Effect of Emotion on Cue Utilization and the Organization of Behavior. Psychol. Rev., 1959, 66, pp. 183-201.
- Goffman, E. Encounters. Two Studies in the Sociology of Interaction. Indianapolis: Bobbs-Merrill, 1961.
- Hyde, R. W. Psychological and social determinants of drug action. In Dynamics of Psychiatric Drug Therapy, ed. Sarwer-Foner, G. J. Springfield: C. C. Thomas, 1960, pp. 297-312.
- Kornetsky, C. & Humphries, 0. Relationship Between Effects of a Number of Centrally Acting Drugs and Personality. Arch. Neur. Psychiat., 1957, 77, pp. 325-327.
- Leary, T. How to change behavior. In Nielsen, G. S., ed., Clinical Psychology; Proc. XIV Intern. Congr. Appl. Psychol., Copenhagen: Munksgaard, 1962. Reprinted in Bennis, W. G., et al., Interpersonal Dynamics. Essays & Readings on Interpersonal Actions. Homewood, Ill.: Dorsey Press, 1964.
- Leary, T., Litwin, G., Sc Metzner, R. Reactions to Psilocybin Administered in a Supportive Environment, 7. Nerv. Ment. Dis., 1963, 137, pp. 561-573.
- Leary, T., Metzner, R., Presnell, M., Weil, G., Schwitzgebel, R. 8c Kinne, S. A Change Program for Adult Offenders Using Psilocybin. Psychotherapy: Theory, Research and Practice (In Press, 1965) .
- Linton, H. B. & Langs, R. J. Subjective Reactions to Lysergic Acid Diethyl-amide (LSD-25) . Arch. Gen. Psychiat., 1962, 6, pp. 352-368.
- Malitz, S., Esecover, H., Wilkens, B., & Hoch, P. H. Some Observations on Psilocybin, a New Hallucinogen, in Volunteer Subjects. Cornprehens. Psychiat., 1960, r, pp. 8-17.
- McNemar, W. Psychological Statistics. New York: Wiley, 1955.
- Nowlis, V. Sc Green, R. F. The Experimental Analysis of Mood. Paper presented to XV1h Int. Congr. Psychol., Brussels, 1957.
- Rinkel, M., DeShon, H. J., Hyde, R. W. Sc Solomon, H. C. Experimental Schizophrenia-like Symptoms. Am. 7. Psychiat., 1952, rob, pp. 572-578.
APPENDIX B: DESCRIPTION OF THE MAIN EFFECTS
Below are listed some sensations and experiences that people have had under this drug. We are interested in your reactions to the drug. Please mark each one according to the following scheme:
0 - did not occur
1 - occurred once, or only a little
3 - among the most important aspects of my experience
49. nausea
50. dizziness
51. weightlessness
52. looseness of limbs
53. eyes and nose oozing
54. heaviness
55. numbness
56. hot
57. cold
58. lack of balance
59. trembling
60. throat-chest constriction
61. headache
62. bodily pleasure
63. body melting
64. inexplicable laughter
65. blocking of speech
66. loss of time sense
67. colors more intense
68. contours more intense
69. visual after-images
70. objects distorted
71. floors, walls, objects, etc. moving
72. distances changing
73. objects more significant and beautiful
74. seeing the fine, detailed structure of things
75. people's faces more significant and beautiful
76. self or other people changing size
77. sounds, music moving around the room
78. unusual odors or scents
79. connection between visual images and music
80. connection between music and thought
81. music more beautiful and significant
82. visions of abstract geometric patterns
83. visions of buildings or parts of buildings
84. visions of flowers, trees, plants, animals
85. visions of whole landscapes, oceans, mountains, deserts
86. visions of fabulous animals, monsters, unique creatures
87. visions of heroic figures, such as angels, God, devils, superman
88. visions of people known to you personally or publicly
89. visions of waves, water, fire, stars, planets, rockets, meteors
90. passing through stages of evolution
91. travelling in exotic places
92. visions of utopias, cities of the future
93. witnessing historic events
94. feeling no separation between self and the visions
95. being able to manage and control the visions
96. feeling that objects or events in the environment have some direct peculiar relation to your life or your problems
97. feeling of being at several different levels
98. being passively at the mercy of the visions and hallucinations
99. feeling of flying or gliding
100. rising
101. falling
102. swimming, floating
103. chasing
104. being chased
105. vision of exploring, following a guide
106. being beaten, tortured, or devoured
107. eyes staring at you
108. feeling of disintegration,
falling apart
109. feeling that you were going to die
110. fantasy of going back into the womb
111. fantasy of being born again
112. thoughts and ideas flashing by very rapidly
113. feeling of being very wise, knowing everything
114. seeing great significance in ordinary statements or remarks
115. being able to solve problems with ridiculous ease
116. sense of confusion, incoherence, irrationality, chaos
117. sense of omnipotence
118. sense of absurdity of one's thought and speech
119. being able to operate on several levels at once
120. feelings of unity of all things
121. being part of a larger unity
122. close bond or contact with God
123. feeling of insight into self, without being able to state what it was
124. insight into self that is describable and lasting
125. feeling of bond and closeness to a particular individual
126. feelings of unity of the whole group
127. preocupation with people coming and leaving the room _
128. seeing significance of people's actions and movements without verbalization
129. suspicious and resentful of people not taking the drug
130. wanting to communicate but not being able
131. wanting to tell the whole world about this experience
132. fear of being thought silly or stupid or crazy
133. feeling left out or isolated
134. fear of losing control, of going insane
135. vague feeling that some outrage might happen
136. unusually talkative
137. easy understanding of others' feelings
138. sharing and communicating thoughts without words
139. wondering about the effects of the drug
140. fighting the oncoming effects of the drug
141. anxious about having to come "out of it"
142. feeling of "I knew that it was going to happen"
143. seeing symbolic meaning of things
144. seeing unusual uses and connections between ideas and things
145. finding God
146. feeling beyond good and evil
147. confronting the mystery of life
148. love and brotherhood for all mankind
149. feeling that nothing need be said
150. extreme pleasure, ecstasy, cosmic joy, paradise
151. sadness, grief, sorrow
152. depression (i.e. blankness, stupor)
153. explosive anger or fury
154. terror, panic, wild fear
155. large swings of mood, happiness and sadness
156. absence of feeling or emotion (abstract thought only)
157. complete mental calm, peace
APPENDIX C: MAIN EFFECTS CLUSTERS
I. Somatic Symptoms: #49-65
II. Perceptual Transformation: #67-81
III. Hallucinations (perpetual) : #82-89
IV. Hallucinations (involving whole person) : #90-95, 98-111
V. Unusual Cognitive Phenomena: #66, 96, 97, 112-120, 130, 142-144
VI. Religious, Mystical: #120-122, 145-149
VII. Interpersonal-positive: #125, 126, 128, 131, 136-138
VIII. Interpersonal-negative: #127, 129, 130, 132-135
IX. Drug Concerns: #139-141
X. Primary Processes: #63, 66, 95, 96, 98, 116, 117, 143, 144; all II, III, IV
XI. Paranoia, Ideas of Reference: #96, 106, 107, 129, 132-135
XII. Empathy (insight) : #123-126, 136-138
Download Our Free Psychedelic Healing Books